Serving her purpose: Sara Harris inspires students, staff at Calera Elementary School
Published 1:18 pm Tuesday, March 19, 2024 By Alec Etheredge
Calera Elementary School teacher Sara Harris continues to inspire her students and peers as she continues to work her dream job despite battling cancer.
Standing front and center in her classroom with a room full of students wide-eyed in anticipation, Calera first grade teacher Sara Harris breaks out in a dance. The students quickly follow suit, some with giggles at their teacher, but all with one goal in mind—retaining knowledge through interactive lessons at the hand of their teacher.
Through the fog of the boisterous environment of singing and dancing, you don’t see the pain of a teacher with an incurable metastatic breast cancer, and that’s exactly what Harris hopes for. Diagnosed with breast cancer for the first time in 2019, the first grade teacher had it return in metastatic form by spreading to her sternum in 2021 when she got her dream job at CES. Her focus, however, remains on the students, fighting through the painful days to serve her purpose and not let the cancer define her.
“I absolutely love what I do,” Harris says. “I feel like it’s my purpose.
The best part of it is the children.
It is a joy to walk into this room every day, no matter how tired I am, no matter how I feel, sometimes I walk in and go, ‘Oh, I can’t do this today,’ and when they walk in that door, it wipes all of that away. Watching that lightbulb moment, it’s just so exciting to watch them learn and grow.”
For that reason and her engaging method that she continues to bring into the classroom each day, the hometown Calera girl was named this year’s Teacher of the Year at Calera Elementary School, giving her even more clarity on her path.
Finding her path
It was actually Wonder Woman who set Harris on the path to becoming the teacher she is today, and no, not Lynda Carter from the TV series, but a Calera Elementary School kindergarten teacher who looked like her and treated her students in a fashion that made them look at her like a superhero.
“She poured time into me, she invested in me,” Harris says. “She would braid my hair during recess and just show me how much she cared. I thought she was Wonder Woman. She looked like her and everything about her just seemed super. It wasn’t every day the original kind of thing, she went the extra mile.”
She says that was the start of her growing a love for education that grew with each teacher she had through high school.
“They saw things that I didn’t see in myself,” she adds. “It would inspire me to push myself further because I was extremely shy. They would tell me, ‘No, you can be president of this or you can give a speech on that topic.’ I wanted to be that for children also. I wanted to pour that into students and other people as well. That became what I had to do.”
After graduating from Calera High School in 1993 as part of a class of 44 students, Harris went to college off and on and had her three kids before graduating with a degree in education. Originally, she didn’t plan to return to the once small town of Calera.
“At first, my sister was a teacher at Calera Elementary, and I thought to myself, ‘Why would anyone want to go back to their hometown?’ But, through the years, there is just something about this town,” she says. “There is such a love for community and still a small-town feel even as it grows.”
Harris went on to teach fifth grade, third grade and fourth grade in that order at Calera Intermediate School, but her heart continued to pull her back to younger children. That led to her taking an opportunity at Randolph Elementary School as a first grade teacher to gain experience. But then, a kindergarten job opened at Calera Elementary School and she couldn’t pass up the opportunity to chase down her dream.
“I went here, my children went here, my grandchildren will go here, so it’s part of my legacy to continue pouring into this school and this town because I want this community to keep growing and for these kids to keep pouring into the community,” Harris says.
Now in her 12th year as an educator, she has spent the previous two years teaching first grade at CES after serving as a kindergarten teacher in 2021. She had her dream job at her dream school, but it didn’t come without its challenges.
A detour around the roadblock
As the 2021 school year approached, Harris was giddy with excitement after being hired to take on a kindergarten teacher role at Calera, helping her dream become a reality, while her cancer, to her knowledge, was gone. Then, a week before the school year officially began, Harris got the news that her cancer had spread to the sternum on Aug. 6, 2021.
“It was gone in a sense. I had kind of beat it because it wasn’t showing up in my bloodwork,” Harris says with tears filling her eyes as she remembers the challenging time. “It was so ironic. It was my goal to be here and I find out that my cancer is back at the same time I’m about to start my dream job.” In that moment, while difficult, she didn’t panic and very quickly told first-year principal Shannon Montgomery what was going on and that she didn’t want the cancer battle to define her, rather that her focus was on making a difference in the lives of the students and living out her dream.
“She has been very open with me about it since the beginning and has never wanted it to define her,” Montgomery says. “A lot of people could have said, ‘I just can’t handle all of this,’ but she said, ‘I want to be here as long as I can be here.’”
Through the adverse situation
She never lost sight of the students and she has rarely missed any days that weren’t for doctor appointments, fighting through exhaustion, pain and mental hurdles to be there for the kids on a daily basis. “Even when she is out of work, she is constantly concerned about what they need to have to be able to succeed,” says co-worker and first grade teacher Hailey Dolbare. “She is currently battling cancer in her sternum—taking chemo meds and going to multiple doctor appointments—all while she is going above and beyond in the classroom.”
A big reason for the ability to push through, in addition to her drive to make the kids her main priority, has been leaning on her faith and the community support. “Faith plays a huge part in every part of my life,” Harris says with tears streaming down her face. “It is part of who I am. It’s part of how I respond to them as children, it’s part of how I respond to my co-workers, it’s part of how I respond to conflict, when I’m irritated. It drives me and I see something beyond what’s here.
My goal is to hear Him say, ‘Well done.’”
Currently, that’s what keeps Harris going on a daily basis, knowing that her purpose is to make a difference for the kids. “It keeps me going, but I also believe if I’m going through this, there has to be a reason,” she says. “It’s either something I have to learn or someone around me has to learn. Cancer has transformed me physically, but it has also transformed me as a Christian and a person.
Things that used to seem like a big deal to me aren’t a big deal anymore because they really don’t matter. In the grand scheme of things, my purpose on this earth is whatever he has placed on my life, and right now, it’s pouring into this classroom and these children. I feel like each child that is in here is in here for a reason and they’re handpicked to be with me for a reason. Each morning, when we have a moment of silence, I pray over them. They don’t know that, but I pray over them and pray over this school for protection around it and that I will be a positive light in their life.” It’s that quality that rubs off on the staff and students around her, as they see her working for something bigger than herself.
“Knowing her personally, she is always respectful of people and their views, but she is very vocal in her faith to us as a staff and that is an additional part of who she is,” Montgomery says. “I see that in her. She is very committed and relies on that heavily. She looks to that for strength as a teacher and day to day life, but also the journey she is going through in life. She extends grace.”
Dolbare echoed that sentiment, saying it’s inspiring to see the strength she gains and the grace she has through the challenges. “She will always tell you, ‘This is not my story, but His story,’” Dolbare says. “When you talk to her about her journey, she tells you that Jesus is right there in the midst of it. She constantly turns to Him. Does she have not so great days? Absolutely! But she keeps fighting every single day and her Eagles’ family rallies around her every step of the way. She is a literal angel on Earth. Heaven will be bigger because of Sara constantly sharing her unremarkable faith throughout her cancer journey.”
Serving her purpose
Standing on top of tables, teaching a fifth-grade class at Calera Intermediate School.
Harris and her students join together in singing songs at the top of their lungs. Another interactive activity, she is trying to make sure her students can remember this song to help retain the knowledge. “I’m not a great singer, but they go along with it,” she says. “I can’t get on the desks anymore because you don’t want the little ones to fall, but when we sing those songs, they remember them. They know what to do. I want them to come in and think learning is exciting.”
Even though she isn’t jumping up on desks anymore.
She continues to sing to her best ability, while also working to create other fun activities that include Math Easter Egg hunts, circus days to celebrate learning, transforming her room into a restaurant for “book tastings” and so much more.
“When I shut that door, I will do whatever it takes to get their attention for them to learn,” she says. “I want them to come in and think, ‘What’s next?’ I want them to have a core memory of this is why I know the doubles like two plus two equals four.”
She says she knows it’s her job to do everything she can for the kids because that’s the purpose she is meant to serve. “They refill me and don’t just see me as someone with cancer,” she says. “I know there have been times that they have to listen to me say I don’t feel good, and they encourage me to keep going, but I try not to even tell them that. I just want to be there to give them all I can and make sure they have a fun day of learning.” It’s a presence that carries from outside the classroom to start the day and into the classroom throughout the day.
“Her classroom is one of the happiest, most welcoming rooms in our building,” Dolbare says. “She meets all of her children in the hallway with a smile and a hug. She is constantly coming up with ideas on how to engage her students and sharing those ideas with all of our grade level. She is seriously one of the most helpful people you will ever meet.” Montgomery says that the kindergarten through second grade years are so instrumental, and having a teacher go the extra mile like Harris is something that can set a student up for success for the rest of their education journey.
“She wants to make learning fun,” Montgomery says. “Getting to know her, what sticks out, is she is very dedicated. It’s so easy to kind of just give up and not show up for different reasons, but she shows up and when she’s here, she’s in it for these kids. We always have to teach to the standards. That’s what we always hear in education, but the fact that she takes that extra step to say, ‘Hey, what can I do to make this impactful to the kids?’ Standing on the teacher table, hanging bats from the ceiling just because she was setting up for that learning unit and just giving the kids that little surprise when they walk in the room. That not only makes it fun, but it sticks.”
Fulfilling her dream
Passing Harris in the hallway one afternoon in the early part of the 2023 school year following dismissal, Principal Montgomery told Harris to come by her office in 10 minutes. Immediately assuming the worst, Harris began the trek to the principal’s office that we all feared as children, but the news wasn’t the terrifying dream she had made up in her head.
“She thought something was wrong and I knew she would think that,” Montgomery recalls. “She came in and sat down, I had my serious face on and started off with something vague. Then, I just blurted out, ‘You’ve been named Teacher of the Year! She immediately burst out in tears.” Harris was in shock. She downplayed it and questioned Montgomery through her tears, saying, “Are you sure. I don’t deserve that.”
“It reminds you that everything you do, people are seeing,” she says.
“It sounds ugly, but I’m not doing it for them.
I’m doing it for God and these children. But, it meant a lot for others to see something in me that they thought I deserved. I don’t feel like I deserve it, but it is greatly appreciated and it means a lot to me.” Montgomery says that is just part of her humble nature and that she continually said that it surely couldn’t be her.
“A lot of times, when you’re doing something good, you don’t really see it and it takes somebody else to see it and that was her,” Montgomery says. “She downplayed it and said she isn’t doing anything special. They see who she is, they see her as a person and a teacher and that is all a part of being Teacher of the Year.”
For Harris, however, it’s all about giving everything she has to the students because that’s the job she dreamed of. “Some days are harder than others, but every time I walk in this door, the pain is gone,” she says.
“I don’t think I’ve ever missed a day because I don’t feel good. I’ll get up and may not be feeling it that day but keep moving forward because they need me to give them 110 percent, so that’s what I do. If I don’t have my all to give to them, they’re not going to get it.”
With that, it’s a medicine unlike anything else that helps Harris get through the difficult times. Seeing it click with her students and seeing their love for her is the driving force that inspires her to be the best she can be.
“Their joy about learning, their happiness to see me and the way they love me, it just makes you feel so good and excited about your day,” she says. “Knowing they need me to teach them and they need this, especially in first grade being such a big building block on their education, makes it all worth it.
Their smiles, their joy, their happiness to be here and to learn, it makes me feel incredible. It brings me happiness to see their little faces.” From the kindergarten student who was inspired by her teacher to pour into others to the Teacher of the Year at that same school, Harris is now pouring into others to make a difference in the same facet, and she isn’t letting a terrifying disease keep her from inspiring students the same way she was inspired at the same age.
“According to doctors, the cancer will never go away, but I will work until the half day of my funeral, I can tell you that much,” Harris says. “I will be here as long as I can physically come to school and do it. That could be five years or 15 years. I’m going to keep doing it because I love it and I’m not going to let something like that stop me.” Calera Elementary teacher living her purpose, inspiring students despite living with incurable cancer (wvtm13.com)
The Day Covid 19 Hit Our Shore was equivalent to The Normandy landings were the landing operations and associated airborne operations on Tuesday, 6th of June, 1944 of the Allied invasion of Normandy in Operation Overlord during World War II.
On June 6, 1944, thousands of Allied servicemen landed on the shores of northern France with a mission to free western Europe from Nazi tyranny. Over the ensuing hours and days, the men faced decimating machine-gun fire, mortars and artillery, eventually fighting their way inland, but not before suffering a staggering number of casualties.
Codenamed Operation Neptune and often referred to as Deployment or D-Day – Search Videos (bing.com) it is the largest seaborne invasion in history.
Baffled by the amount of people who so easily masked their faces, closed their businesses, and took a jab because the government said so, Gianna began studying the difference between rules, codes, and statutes during the pandemic which are not laws.
What happened to our Constitutional rights?
There’s not a college you can attend to gain this knowledge, and the common law is not taught in law school. One has to study Supreme Court rulings in addition to a lot of trial and error to fully grasp the power “of the people”.
Gianna has been studying this since the inception of the pandemic which has made her a self taught Constitutional rights and common law expert.
Her weekly online program, theInalienable Show, exclusively on Rumble, is co-hosted by Scott Bernard, a law school graduate who chose not to join the BAR, but instead, had his eyes opened wide by the difference between statutory law and common law.
When she met Scott who has expertise In Corporate Commercial Law, Uniform Commercial Code, and Domestic Banking Law, she began studying under him and his unique knowledge, and just like Scott, she learned that she had already been living “in the private” for over 25 years.
Together they crafted an online membership, called the Inalienable Universitywhere they teach people that their rights are INALIENABLE, and how to exercise them in their daily lives.
They teach how to acquire the lens at which to decipher the fraud and deception of government contracts such as the driver’s license, state registration, and recording your private property with the county, thus putting you “in the public”.
It’s no accident that civics is rarely taught in school because free people are a danger to the government’s out of control spending. 99.9% of people have never ever been taught how to exercise their rights and freedoms and unfortunately, blindly follow orders.
Gianna and Scott’s curriculum will change the way you walk in the world.
Look at the state of the world. There are still people wearing masks in their cars, in the stores, on planes, and in the sunshine. The entire world masked, vaxed, stood on green circles, and believed news that was just fear mongering propaganda. Every facet of our lives has been disrupted.
15 days to stop the spread. Yeah right. Who didn’t know that was a lie? I knew it and I immediately made an appointment to move out of NYC the same day that was implemented.
But ok you’re here now. We’re here now. We are awake on many levels and we want out of the corporate slavery.
Self-determination is the “freedom to choose one’s own acts without external compulsion”. The term is generally associated with the freedom of the people of a given territory to determine their own political status.
The right to self determine dates back to Socrates in 399 BC, and Aristotle in 350 BC, and Cicero if 56 BC, and it took a more prominent position in Vatel’s Law Of Nations in 1758 which states:
“Each individual, moreover, is intimately conscious that he can neither live happily nor improve his nature without the intercourse and assistance of others.”
The U.S. Constitution of 1787 refers to the Law of Nations, twice.
Charles Caleb Colton states that, “Liberty will not descend to a people, a people must raise themselves to liberty; it is a blessing that must be earned before it can be enjoyed.”
And finally, it’s mentioned in the U.N. “INTERNATIONAL COVENANT ON CIVIL AND POLITICAL RIGHTS”, PART I Article 1; All peoples have the right of self-determination, “By virtue of that right, they freely determine their political status and freely pursue their economic, social and cultural development.”
It’s unfortunate that the U.N. of 2022, is now implementing the World Economic Forum’s Globalist Agenda of a one world government, and so far 55 countries have lost their right to self determine because of color revolutions using Dominion voting machines taking over and getting their chosen candidates installed, and the United States of America is on the chopping block having had our 2020 elections extremely tainted with fraud.
If you don’t see that we are in a color revolution in the USA, you’ve been asleep.
We are living in a time of complete lawlessness, and if the Biden regime had a plan to manage the decline of our country, they would be doing everything they’re doing today…..eroding our rights inch by inch. The frog in the boiling water pot.
Stand up now or be on your knees forever.
If that’s not enough to entice you to explore repudiating your US citizenship and becoming a state national, which is what you were when you were born, how about this:
The term “national” means a person owing permanent allegiance to a state according to
Title 8, Chapter 12 – Immigration and Nationality U.S.C. subsection 1101(a)(21).
To reach the Zero Percent tax bracket, a person must realize that they cannot be anything other than a state national listed in the government’s system.
The War Between “We the People” And the BAR Association
The BAR Association is a cause of the vast majority of problems we have in America and the world.
They own and control everything. Who do you think controls every single thing you look at and every single thing you encounter? We live in a time in which we have some of the largest companies that have ever existed in the world.
We’ve got Microsoft, Amazon, Disney, Blackrock, Vanguard. Who do you think controls those? Who do you think controls mom and pop stores? Who do you think controls the government of Washington DC?
Who controls all the little municipalities and county governments?
We the people think that we elect our representatives, and they control the government, and the CEOs make the decisions for the corporations.
No, not one CEO, and not one legislator makes a decision. Not one. Invoices, contracts, brochures, policies, descriptions, every single one of them is not written by CEOs. They’re written by lawyers.
CEO’s don’t make a decision without running it past their legal departments. The BAR Association makes the decisions that run the world.
The truth is, that lawyers and judges barely know they “law”. They don’t know its origin. They don’t know where it came from. What they learn in law school is PROCEDURE.
Where did the law come from? What is its origin? How did we arrive at this thing called law where a small group of men could put something down on paper and try to hold free men and women accountable?
Let’s start with jurisdictions. Most people think of jurisdiction as a physical boundary like their town, county, or state. That’s just part of the equation.
It was in Genesis 1:26 that God gave man dominion over the land, the air, and the water.
The law of the land became common law. God gave all mankind property, its equity, and its rights.
Our rights are “un-a-lien-a-ble”, meaning they cannot place a lien upon our rights. Those rights are unalienable. It has to do with things of property; nature, patents, and grants and securities, gold, silver, commodities, and things we own.
That’s what common law is. It deals with properties. It deals with our rights.
The air is the highest form of law. The air is above the land which is above the water. The air is ecclesiastical, or Canon law, which is trust law. All things held in trust held in the benefit of another; our heirs.
In Genesis 1:26; then God said, “Let us make mankind in our image, in our likeness, so that they may rule over the fish in the sea and the birds in the sky, over the livestock and all the wild animals, and over all the creatures that move along the ground.”
Why did God start that off?
Right in the very beginning of the Bible, he put the world under trust to mankind. We’re the trustees. He’s the executor. He placed it to us to manage for the benefit of our beneficiaries; our future heirs for generations to come, and lives in perpetuity forever.
What is the definition of forever?
Forever has until the end of the earth, that we’re an eternity.
Jurisdiction of the water is admiralty law. It is commerce and contract law; things held in contract with another. Think about when there were ships going across the seas to find, visit, and bring goods to other lands. There had to be things in place for international regulations right? That’s admiralty law.
Probably everyone reading this has signed a contract at some point in their life, having no idea that it was most likely unlawful. There are some interesting elements to a true contract that a BAR Association member doesn’t want to teach you.
The BAR Association teaches you that there’s got to be an agreement consideration.
Both people have to sign and you’ve got a contract.
But one of the most important of those elements is that a contract has to be between like kind. Can a man write a contract with a man? Yes. That means mankind in this context, not gender specific.
So a man can have a contract with a man.
But a corporation has to have a contract with another corporation.
Have you ever signed a contract with a corporation?
Like with a gym? Or a mortgage?
How about your apartment lease?
Or opening a bank account?
We do it every day and we’re probably doing so using our ALL-CAPS name as our corporate entity without even being aware of it. Sometimes we’re doing it with our non-caps name, and it’s not a lawful contract.
Can a man have a contract with a corporation? No. Why did they put things in corporations? To limit liability just to that corporation. Do you as mankind have limited liability? No.
If a man has integrity, purpose, and knows all eight elements of a contract and writes a proper contract where there’s a meeting of the minds, that’s a proper lawful and legal contract.
There’s full and honest disclosure of the terms and conditions of the contract. There’s equal consideration where one person gives something up, and one receives. It has to be a two way street.
So why did government entities recreate themselves as corporations? The reason is because of a lack of integrity. If they had integrity they would never need a corporation.
One of the main things to be learned is that the United States of America is not the same thing as the United States; it is not the same thing as USA Inc.
Intrigued yet?
Gianna has attended media training at the Television News Center in Washington DC, Media Matters in NYC, Patricia Stark private training, and the Connecticut School of Broadcasting.
♫ 700 WLW On-Demand | 700 WLW Cincinnati (iheart.com) Dan talks with Lora Ries of the Heritage Foundation about the border and Biden’s executive order as well as looking back at the COVID-19 Pandemic with Gianna Miceli. Dan also takes your calls and hears your voices.
Ashley is a member of the Auburn cluster & a huge advocate for ocular melanoma & research for years!
Here’s a little snippet of her story:
“I was first diagnosed when I was 42 years old. It was 2012 & I lived in Memphis, TN with my husband & 4 children, the youngest was 7.
I had gone to the beach with family friends. My friend Jill asked me about a black spot on my eye. I hadn’t noticed it. I went into the bathroom & to my dismay there was an irregular black spot on my iris. I showed my husband, whose nickname for me was “Sweet eyes” & he had not noticed it either. I am ashamed to admit I went home & did nothing for about a month. I googled “change in iris color,” but nothing alarming came up.
A month later, on my daughter’s birthday, my husband & I were invited to a dinner party—which we only attended since our daughter was spending time with a friend.
My husband was the administrator for an oncology group in Memphis and the dinner party was at one of the doctor’s house. While there, a friend asked me about the black spot. She had her husband look at it & he strongly suggested I see a doctor as soon as possible.
On Monday I made an appointment with a local Ophthalmologist, but being a new patient it was going to be three weeks till I could get in to see the doctor. I can not believe I am admitting this but I had never had an eye exam except during elementary school. The only “symptoms” I was having was occasional blurriness.
While running errands I saw a large sign outside a “Visionworks” that read, “FREE EYE EXAM” so I walked in & asked for an eye exam. The beautiful young Optometrist did her exam & recommended eye glasses. When she completed the exam I asked her, “What do you think about the black spot on my eye?” She sat back & said, “You do have a black spot on your eye. Let me make a phone call.” She said I needed a dilated eye exam & she got me into Dr. Mathews who was a local Ophthalmologist…& so my story really begins!”
It’s not yet clear what is causing the apparent clusters of ocular melanoma
After noticing black spots in her iris, Ashley McCrary was diagnosed with ocular melanoma. “I was like, ‘Well, I know two people who’ve had this cancer,'” McCrary tells CBS News. To say that’s unlikely is an understatement: Between five and six out of every one million people are diagnosed with the rare eye cancer, yet two of McCrary’s friends also had it; the three attended Auburn University in Alabama together.
Another Auburn alum was also diagnosed; the women started a Facebook page to look for other alums dealing with the same cancer—and 36 people have gotten in touch so far, McCrary tells CBS. According to the page, most of those affected attended Auburn between 1983 and 2001. Last month, WLTZ reported that at least 31 people who attended or worked at the university from 1980 to the early 1990s have been diagnosed with ocular melanoma. Earlier this month, Healthline put the number diagnosed in the area at 33.
Similarly, a number of people in the Huntersville, North Carolina, area have also been diagnosed with ocular melanoma, also known as uveal melanoma. CBS puts the number at 18, while WFAE reports that 23 people who lived, worked, or spent significant time in Mecklenburg County since 2000 have been diagnosed with the disease.
Many of the patients in both areas are young women, Newsweek reports, despite the fact that the disease is typically more common in older people and men. Officials have so far been unable to determine what might be causing the apparent clusters of cases (though the Alabama Department of Health’s official stance is that “it would be premature to determine that a cancer cluster exists in the area”), but doctors in Philadelphia are studying the patients, some of whom travel there for treatment in a clinical trial. Doctors at Columbia University are also studying the tumors of diagnosed patients, and Auburn University has put together a committee to investigate. (More cancer stories.)
“I hadn’t been to the eye doctor since probably elementary school. Before my diagnosis, I had a little bit of blurry vision looking at a computer screen, but it was minimal. I didn’t think anything of it. But one night in 2012, we were out to dinner with colleagues from my husband’s oncology group, and one of the wives noticed a black spot on my iris. Her husband, who is a doctor, took a look at it. He wasn’t alarmed, but said I needed to have it looked at. So I did.
Soon after, I saw an optometrist, who sent me to an ophthalmologist, who sent me to an ocular oncologist. I didn’t even know ocular oncologists existed. We found out I had ocular melanoma, also known as uveal melanoma (UM), in my right eye. So, I had my eye surgically removed. Prior to the surgery, I was told that we were just gonna keep an eye on it (no pun intended).
But the cancer ended up being more serious than we originally thought. After genetic testing, which was fairly new at the time, we learned that the type of UM I had was very likely to come back. I was put on surveillance, with scans every four to six months. Honestly, I felt like I was just going to be that one person where the statistics worked in my favor. And for eight years, my scans were clear.
Things quickly went from being totally fine to not fine
Fast forward to October 2020. Shortly after moving to Auburn with my family, my doctor called and said I needed to come in to talk about my recent scans. They told me I needed to bring my husband Dave with me. I texted my friend, Marlena Orloff, a doctor in Philadelphia I had met through UM research in years prior, and I said “I think we’re getting some bad news. They told me to bring Dave today, and that hasn’t happened before.” Things quickly went from being totally fine to not fine.
During the appointment, the doctor showed me an image of my liver. It was black with white dots all over. We called it starry night, as if we were looking up at the night’s sky and seeing the stars. Except the stars were 100 tumors. We knew then that my cancer had metastasized, and that nowhere in Alabama offered the treatment I would need.
The places you’d go would of course be Thomas Jefferson, Columbia, Sloan Kettering, Duke, MD Anderson, & UCLA. So, I was really lucky that I already had a relationship with the doctors in Philadelphia. Within a week we had a plan. Everything happened so fast. This isn’t the typical scenario. Usually it takes 6 to 8 weeks to get an appointment, and then another 3-4 weeks to figure out your treatment. I was very fortunate.
The doctors in Philadelphia did a biopsy and looked for genetic markers. Not all doctors would have known to look for those markers – they were just buzzwords for most at the time – so again, I was very lucky. They found I had two markers indicative of aggressive cancer. I started with Immunoembolization (IE) for 8 months, and was also moved to the top of the clinical trial list.
That way, I had time during my initial treatment to learn about the clinical trial, ask questions, process it, and be ready to make a quick decision if IE didn’t work. And sure enough, in May, we found “innumerable new tumors.”
Normally when you’re diagnosed with metastatic disease, you have about a year, year and a half to live. And since my cancer is so rare (6 out of 1 million people are diagnosed per year), there aren’t many treatment options. So the idea of being on a clinical trial that could potentially work – and was working – was very, very encouraging. I was ready to sign the papers.
But Dave was more hesitant. He said, “Wait a minute. The second person died in this trial. Can we talk about that? You’re going to be a human experiment. You know that, right?” He was hopeful for a more conservative approach. But I was ready to go. We had read the material in advance. We were prepared. But when it came down to signing the paper, his hand was trembling. It’s hard. He’s really just a beautiful soul.
To Dave’s point, in the early days of the trial before I joined, the first participant responded really well. Her name was Summer. She was in her mid 20s and was a friend of mine. But the second person, she was in her 70s, and after taking her first dose, she died the next day. So, they had to stop the trial and figure out what happened. This meant that Summer’s treatment stopped.
Unfortunately, she had no other options, and so she passed away. That was really hard. It turns out that the older woman died from a heart attack. She had comorbidities that she was unaware of. I was fortunate, because by the time I was ready to join the trial, they had already restarted it. 15 people were on it and were doing really well. So that made the decision easier for me.
I’ve never experienced pain like that in my life
I arrived for my first day of treatment in Philadelphia on a beautiful day in July. I was in a cute sundress. Normally you have to change into a gown and lay in the bed and get your treatment. They told me I didn’t need to change my clothes, I could just hang out. I had friends who came by to cheer me up.
So I was in my cute dress, with my cute friends, and my cute husband. I tell you this because it just felt very relaxed and casual. There was not a whole lot of stress about it. The doctors came in and gave me the infusion, and still within two hours I was feeling great.
During this time, a friend of mine took a picture with me, and I have a smile on my face. But within minutes of that picture, I went from 0 to 500 pain. I’ve never experienced pain like that in my life, and I’ve had four children. It scared everybody. Emergency teams were coming in.
I couldn’t lay in bed or sit up. I knelt on the ground with part of my body on the bed, in my cute sundress. My husband was trying to rub my back because that’s where the pain was so bad. The doctor came in and said the only reason my back would be hurting that bad was if the treatment was attacking a tumor in my back or kidneys (we found out later it wasn’t a tumor, it was just a painful response to treatment that only happened the first time). He was completely perplexed as to why I was in so much pain. It was very scary.
It felt like five years of intense pain before I got morphine. Four hours later, the real symptoms kicked in: fever, shakiness, joint and back pain, and a dip in blood pressure. This would eventually happen like clockwork every time for 6-12 weeks. I got pre-drugs moving forward. Once I got through the initial dose escalations, it became an outpatient infusion. So I fly to Philly once a week for my infusions and stay in a hotel with a plethora of medicine with me, since I know what to expect with side-effects. I’ve now done this 94 weeks in a row.
My results have been shared all over the world
Other people have responded well to treatment, but I had a miraculous response over a period of time. I went from over 100 tumors down to 10. And then from 10 down to six. Two of my target tumors had shrunk 50% in size. My results have been shared all over the world.
Eventually, though, we found that one rogue tumor had grown, and it’s not easy to get approval to stay on a trial if your disease progresses. The trial sponsor didn’t want me to continue with it, but my doctor really pushed for it, because they knew the treatment was working for all the other tumors. It was just that rogue one, which they could treat with radiation.
So I got permission to stay on the trial for five more weeks, but my latest scans have shown that more tumors have started growing again and I have a growing tumor in my lung.
So, I’m at a pivotal point now. I’m in my third week of being treated beyond progression. My scans are on May 31st, and we’re supposed to come up with a Plan B, because I may not be approved for the trial anymore.
There were 16 people in the trial to start. Now there’s only seven. Some people had disease progression and passed away, some had trial burnout. Some couldn’t afford it. There are only a few places in the US you can go for treatment. There’s just not a whole lot of people who can do this once a week, every week, for the rest of their lives. To fly there every week, stay at a hotel, get Ubers, meet with the nurse practitioner…it’s very expensive. There’s a lot the trial will pay for, but it doesn’t cover everything and they don’t pay for someone to come with you.
I kind of have what they call survivor’s guilt
My situation is extremely uncommon. I’m a unicorn when you consider I don’t have a financial burden in all of this. Through a divine encounter at work, I met representatives from Aflac and ultimately learned I qualified for their cancer plan. So, Aflac really bridges the gap in terms of what the Sponsor pays and what I have to pay out of pocket.
Aflac even covers for a person to go with me to Philadelphia every week. I wouldn’t be able to do it without them. But no one else on the trial has a cancer plan like I do.
So I’ve seen financially how people have had to drop off the trial because they just couldn’t afford it anymore. I’ve seen where people used to have someone come with them but can’t anymore because it’s too expensive.
So, they don’t have a secondary person to be there if anything bad happens. It would be scary to navigate that alone. I kind of have what they call survivor’s guilt. I see people who follow the typical statistics and pass away WAY too young because they just don’t have options.
There are people who would give anything to be on the trial I’m on, but the trial’s not accepting any more UM patients right now. Part of that is because the drug they’re testing (Prame) is working on other cancers as well, and since another treatment for UM was recently FDA approved [Kimmtrak], they closed the trial to UM patients. I’m just lucky I have options.
Before my diagnosis, I learned some tough lessons from friends who had passed away
One of them was such an optimist. Even when the doctors were telling her she had two weeks to live, she was still optimistic. The doctor encouraged her to tell her children about her prognosis, but she didn’t. So, things were left unsaid. They never talked about her funeral. It was very hard on her husband.
My other friend had a lot of unresolved relationships. Pain and regrets and people who needed to be forgiven. So, when I was diagnosed, a light switch went off. I wrote each of my four children a letter…you know, just things you want to say. I had people in my life I needed to forgive, and others from whom I needed forgiveness.
I wanted to handle it all the right way. My husband gave me perspective though. He reminded me frequently, you’re not dead yet, be thankful for today and LIVE! He was right, but I wanted everyone to be keenly aware of my prognosis.
My whole attitude has been, if this is happening, it’s for a reason. I knew God had a plan and purpose for my life. So instead of feeling sorry for myself or crawling in a hole, I look at everything as an opportunity and think, how can I use this to make a positive impact?
How can I live this out with grace?
I just look for opportunities in every single detail of every single day. I see the same servers at every single restaurant I go to when I’m in Philadelphia. I have the same Uber driver who takes me to the airport each week. His name is Geurino. He’s from Haiti. And he sometimes impacts me more than my doctors do.
The way he prays for me and the way he just speaks over my life is very tender and endearing. And the people who go with me to Philadelphia…there’ve been a lot of them. They see what I see, are impacted by it, and then they come back and use it to impact other people. It’s just this whole butterfly effect.
They also see the reality that it is okay to not be okay all the time.
This situation can be very heavy. People will ask where I get my strength from. I always say my strength comes from God; I could not do it without Him. All I can try to do with this cancer is look for opportunities to be positive, to be optimistic but not naive, to be real, to be transparent.
It’s important to have levity and laughter
My birthday is this week. Mother’s day is this week. All of my children and my daughter-in-law are coming to town, which doesn’t happen often. I didn’t ask for it, it was planned behind the scenes because they all understand that this might be a tricky year. We also have a big trip planned this summer. We don’t do stuff like that. So there’s a heaviness to it. We’re just trying to enjoy each day. We’re not suppressing it – we all have addressed what’s happening – but there’s a Southern saying: “don’t borrow worry.” We don’t know what’s going to happen later. I mean, I could live to be a hundred. Who knows. I don’t want to go into it thinking this will be my last Mother’s Day, because I want to be happy. But it’s all still very sobering.
It’s important to have levity and laughter. Dave provides that for me. The world sees him as an introvert…quiet and stoic. But he’s not that way with me. As recent as two years ago, we would go on dates once a week, and in the car we would do carpool karaoke. I never shared it with anyone or recorded them. It was our little secret. But recently he recorded one for me and shared it on Facebook. He rapped to “The Champion,” by Carrie Underwood and Ludacris, one of my favorite songs. It’s gone viral. He helps us laugh even when things are hard.”
We first connected with Ashley in May of 2023. Here’s an update since then:
June 13, 2023:
“Today Dave and I will be leaving for Philly for a new adventure in my battle against Ocular Melanoma. This will be my 99th trip for the Prame treatment but this week we will be adding Tebe (or Kimmtrak) to help fight the cancer that has now spread to my lungs. I am so thankful I have an option. I will go in the hospital for this treatment on Wednesday morning and will discharge Thursday. We will fly back that night. Then I will do these two more times before moving to outpatient weekly infusions.
Just this week I had two friends pass away, Dustin Alinger a week ago and just a short time ago today… my friend Clay Butler. They both ran out of treatment options. With a rare cancer that has no cure, options are few.”
October 11, 2023
“So excited to share the reports from my MRI and CTs. Dave and I found out late this afternoon. Both scans showed either stable tumor in my liver and lungs with a couple of tumors that shrunk! There were also NO new tumors which is so exciting. I found out there is a 1cm nodule in my right breast that was there before and it is unchanged. We are thrilled with this report and completely humbled as we believe the confidence we have is in God through the treatment he has provided through my team in Philly.
This is a huge win for us.
We are once again able to exhale and continue treatment for 12 more weeks!! I recognize what a gift this is since many don’t have the options or outcomes I have. And I am so thankful for Immunocore, the sponsor of both Prame and Kimm Trak. They are the reason I’m alive.
This is a picture of two members of my team… my amazing husband and my main nurse Christie Muldoon. I couldn’t do it without them.
Inspiring Strength
To relieve stress, in 2023 Ashley started waterColor painting: How could I blend my love, passion and desire to help other people she wondered. The answer came in the form of painting Bible verses that have inspired her, along with bright flowers and cute animals, and selling the cards — with all the proceeds going to help fund other patients’ trips for treatment.
Ashley ended spreading the word on social media and created a website EyeonGrace.com benefiting people with Ocular Melanoma needing travel assistance and, soon people were contacting her wanting to buy cards to help themselves or a loved one going through a troubling situation or challenging situation..
Before long Ashley was helping other cancer patients raise money for their own treatments. Today Ashley’s cancer is stable and she has sold over $10,000 worth of cards, which also includes non religious cards, such as, birthday cards. I love being able to help others and gives me a sense of purpose, knowing I am helping others in the same situation she went through and doing good in the world.
“I think it’s sometimes harder for the caregiver than the person in treatment. My husband loves me so much, but he can’t fix this. So he has this helpless kind of feeling. The support he needs is different from what I need. And if you don’t get that support, if you’re not careful, you’re going to hit a wall.
Because there’s this heaviness all the time, every single day. I get to just focus on me, but he has to focus on everyone plus his job. It is a lot to deal with. It’s been almost three years of treatment and I still get cards in the mail almost every day, while Dave’s dealing with work, the emotions related to what I’m going through, and the general stress of life.
He has compounding issues trying to take care of everyone else. So I look for opportunities for him to have time with his friends. And my kids…it is rare that anyone is ministering to them about all this. So when people say, Ashley, what can I do for you? I say if you want to minister to me, minister to my family. I don’t need the Chick-fil-A gift card, but they do.
We are also big advocates of therapy.
Dave has been a few times and it’s really helped. He has the opportunity to meet with other men through online support groups who can encourage him. I just really feel for the caregivers. They didn’t sign up for this. It is so important that their needs are met too and often their needs are greatly overlooked.”
Natasha Allen never planned to go viral or have more than 146,000 followers on TikTok. In 2020, when she was 23 and first diagnosed with synovial sarcoma, a rare soft tissue cancer, it was the height of the COVID pandemic. She’d been on TikTok for a few months, but she was more of a watcher than a poster. That changed when she was staying in the hospital to receive chemotherapy. Allen was lonely and bored and started making videos to entertain herself.
TikTok quickly became a source of community.
“When I started with TikTok, I felt like I was the only one, and being able to post and see comments of people saying ‘I went through this, too’ and ‘This happened to me,’ it makes you feel less alone,” Allen tells Yahoo Life.
She now uses her platform to help educate others.
“I like spreading awareness because, one, not everyone knows about the intricacies of cancer because you only see the romanticized version on TV and in movies, and, also, my cancer is rare, so I wanted to raise awareness for sarcomas because it does affect young people the most,” Allen adds. Allen also hopes the videos she posts help people understand what it’s like to be in your 20s and battling a disease that you never expected to have at all, especially so young.
Dear Lord, please give her the courage to keep fighting, you are the healer of the universe and I wish Natasha going forward that the gift of continued quality of life for many many more years to come is in the cards for you. Keep fighting and thanks for sharing your story.
Thinking of you…oh beautiful one!!! My niece had cancer 6 years ago, she literally came back to life from the brink of death. I visited her every weekend for a year. I have to say being part of that experience has made me more emotional. In general, some people’s episodes of their life are just nonsensical! And if you don’t accept this B.S. life challenges might emotionally/spiritually kill you–it is such a tough experience. And I felt emotionally exhausted and I was just a stand-by. Furthermore in my niece’s situation Cancer robbed her of her fertility but at least she is alive, with long, thick afro hair up to mid back length! And I hope every woman of child bearing age, if possible, is always given the choice of freezing healthy eggs. Her Cancer when discovered was too advanced so she was never given the choice. I am ranting now….I really hope you come through! And you lead a good future!
Literally everything she said is facts. Down from the “for-lifer” friends disappearing on you to you feeling disconnected from your healthy peers and loneliness. I hope and pray she reaches full recovery in Jesus name.
In the name of Jesus I speak healing into your life, I speak divine healing into your life and command that infirmity to flee from you this instant in the name of Jesus!!! Amen…God’s got you girl you are healed this instant… Amen!!!. God is bigger than that battle Hallelujah
I hope and pray she reaches full recovery in Jesus name.
Cancer is a complex and emotionally charged experience, both for the person diagnosed and their loved ones. While it’s essential to recognize that not everyone turns their back on cancer patients, there are several reasons why some people may distance themselves or struggle to provide support:
Fear and Helplessness:
People who haven’t faced cancer themselves might feel overwhelmed by the situation. They may not know how to talk about their feelings or offer meaningful support.
Witnessing a loved one’s suffering can evoke feelings of helplessness, leading some individuals to withdraw rather than confront their own fears.
Guilt and Burden:
Cancer patients often feel guilty about the impact their illness has on family and friends. They may distance themselves to reduce this burden.
Conversely, patients who usually focus on helping others may find it challenging to receive help themselves.
Privacy and Emotional Avoidance:
Talking about cancer can be deeply personal and emotionally distressing. Patients may avoid interactions to prevent discussing their private, upsetting situation.
Some patients lack experience in expressing their emotions, especially when it comes to discussing their own feelings.
Protecting Others:
Patients may pull away because they fear upsetting their loved ones. When they talk about their illness, they may end up comforting the listener, which can be uncomfortable.
After treatment, patients might feel pressure to appear better than they actually feel, leading them to protect others from their true emotions.
Role Changes and Overwhelm:
Illness disrupts established family roles. Patients may pull away due to feeling overwhelmed by the care they receive.
Caregivers, even with good intentions, may inadvertently pressure patients, leading to a sense of loss of independence.
Alternative Therapies and Control:
Some patients explore alternative therapies, seeking a sense of control over their bodies. These therapies may not have strong evidence but provide emotional empowerment.
Doctors often caution against alternative methods, emphasizing the importance of evidence-based treatments.
Remember that each person’s response to cancer is unique, and there’s no one-size-fits-all explanation for why some people turn away. Empathy, open communication, and understanding can help bridge the gap and provide meaningful support during this challenging journey 123.
Synovial sarcoma is one of the rarest types of cancer. This type of soft tissue sarcoma can arise almost anywhere in the body, including the joints. Synovial sarcoma most commonly occurs in the extremities, particularly in the thighs, knees, feet and forearms. However, it also can occur in the head, neck and trunk.
We spoke with Dejka M. Araujo, M.D., and sarcoma research intern Michelle G. Yeagley to learn more about diagnosis, treatment options and the latest research on synovial sarcoma.
What are common synovial sarcoma symptoms?
At what point should someone see a doctor?
Most synovial sarcoma patients discover their tumor from a lump, and for some, related pain. It’s important to see a doctor if you find a lump or have persistent, unprovoked pain in a soft tissue, such as the muscle of an extremity or from within your abdomen. Synovial sarcoma may also occur in the lungs, so see your doctor if you notice shortness of breath.
Tell us about the types of synovial sarcoma and the differences between them.
There are two major types: monophasic, which is made up of only spindle cells, and biphasic, which is made up of both spindle cells and epithelial cells. There isn’t a difference in aggression or treatment between the types.
Are certain patients more likely to develop synovial sarcoma than others?
We don’t see a clear pattern, but synovial sarcoma can occur at any age, with a tendency to occur in young adults. We also see it in men slightly more often than women.
How is synovial sarcoma typically diagnosed?
Synovial sarcoma can be found in the soft tissues by an MRI, or in the lungs with an X-ray or CT scan. However, an official diagnosis can only be made by a pathologist after obtaining tissue samples through biopsy or surgery.
What can patients do to prepare for an initial doctor’s visit regarding synovial sarcoma?
Do your research. If possible, see a doctor who specializes in sarcoma and works at a cancer center that has surgeons, radiation oncologists and pathologists who also specialize in sarcoma. The first surgery to remove a synovial sarcoma tumor may determine a patient’s prognosis. If the diagnosis was made after the tumor was removed, make sure the doctors got all the cancer out. If you’re still not confident, get a second opinion.
How is synovial sarcoma typically treated?
At present, surgery is the most effective treatment, but radiation and chemotherapy may extend the time before recurrence and metastasis when used in conjunction with surgery.
Is there a risk for metastasis and if so, where?
Yes, synovial sarcoma often does spread to other parts of the body. The lungs are the most common, and usually the first, site of metastasis for synovial sarcoma. Metastasis to the brain, bone, lymph nodes and local organs are all possibilities.
Can you tell us about new synovial sarcoma clinical trials?
MD Anderson has two clinical trials that synovial sarcoma patients may be eligible for. The first is for HLA-A2+ patients with unresectable, metastatic and recurrent synovial sarcoma expressing NY-ESO-1. Eligible patients are treated with chemotherapy and given T cells genetically engineered to recognize NY-ESO-1. The hope is that these T cells will kill the cancer cells.
Another study, which is open to patients with various types of sarcoma, is trying to determine if we can successfully treat sarcoma by combining checkpoint inhibitors MEDI4736 and tremelimumab.
Is there anything else you want patients to know about synovial sarcoma?
Synovial sarcoma can be inactive for a long time before it grows again to a size that can be detected by a scan. So make sure you continue to get your regular scans and follow-ups with your doctor, even if you’ve had no evidence of disease for many years. That way, if your cancer does return, we can find it as early as possible, when it’s more treatable.
“Make sure you get your regular scans and follow-ups with your doctor, even if you’ve had no evidence of disease for many years.”
Synovial sarcoma is a rare type of cancer that arises in soft tissues, often near joints. It can occur almost anywhere in the body but is most common in the extremities1.
What are common symptoms?
Symptoms include a lump and possibly pain. If you have persistent pain or find a lump in soft tissue, it’s important to see a doctor1.
What are the types of synovial sarcoma?
There are two major types: monophasic (only spindle cells) and biphasic (spindle cells and epithelial cells). The aggression and treatment are similar for both types1.
Who is more likely to develop it?
Synovial sarcoma can occur at any age but tends to affect young adults. It’s slightly more common in men1.
How is it diagnosed?
Diagnosis involves MRI for soft tissue or X-ray/CT scan for lungs, but a definitive diagnosis requires a biopsy or surgery to obtain tissue samples1.
How to prepare for a doctor’s visit?
Research and consult a doctor specializing in sarcoma. The first surgery’s success is crucial, so ensure all cancer was removed or seek a second opinion1.
What are the treatment options?
Surgery is the primary treatment, but radiation and chemotherapy may help prevent recurrence and metastasis when combined with surgery1.
Is there a risk for metastasis?
Yes, synovial sarcoma often spreads, commonly to the lungs, and can also metastasize to the brain, bone, lymph nodes, and local organs1.
What about new clinical trials?
The article mentions discussing the latest research and clinical trials, which are essential for advancing treatment options1.
For more detailed information, you can visit the MD Anderson Cancer Center’s article on the topic1. If you’re looking for specific details or have more questions, feel free to ask!
Are there any promising treatments on the horizon for Synovial sarcoma?
Yes, there are promising treatments for synovial sarcoma on the horizon. A recent clinical trial has shown potential for an immunotherapy treatment called afamitresgene autoleucel (afami-cel). This experimental cell therapy has been found to significantly shrink sarcoma tumors in more than one-third of patients1.
Here are some key points about this treatment:
Afami-cel is a type of engineered cell therapy, similar to CAR T cell treatments which is used for certain blood cancers.
In the phase 2 clinical trial, almost 37% of patients saw their tumors shrink after receiving a single dose.
Patients with synovial sarcoma responded to this therapy for an average of 11.6 months.
The most common side effect was low blood counts, and about 71% of patients experienced cytokine release syndrome (CRS), which is a common reaction after cell therapies1.
This represents a significant step forward for patients who have largely exhausted other treatment options. For more information on this and other clinical trials, you can consult with a medical professional or research at specialized cancer centers. If you have any more questions or need further assistance, feel free to ask!
The treatment with afamitresgene autoleucel (afami-cel) is currently under review by the FDA, and a decision is expected by August 4, 2024123. This follows the priority review status granted to the biologics license application (BLA) for afami-cel1. If approved, it would become available shortly after this date.
Here’s a brief timeline of the events leading up to the expected decision:
March 28, 2024: Results from an international phase 2 clinical trial published in The Lancet showed a favorable response for afami-cel in patients with metastatic synovial sarcoma4.
February 1, 2024: The FDA accepted the BLA for priority review1.
The priority review designation is granted to treatments that, if approved, would significantly improve the safety or effectiveness of treating, diagnosing, or preventing a serious condition. This accelerated review process is a positive sign for the potential availability of afami-cel.
Keep in mind that the availability will also depend on the outcomes of the FDA’s review process and any additional requirements that may be set by the regulatory body. It’s advisable to stay in touch with medical professionals or follow updates from the FDA for the most current information. If you have any more questions or need further details, feel free to ask!
Renowned anthropologist, and former Explorer-in-Residence at the National Geographic Society, Wade Davis on the myth of American exceptionalism, and why Donald Trump is “less the cause of America’s decline than a product of its descent.” As they stare into the mirror and perceive only the myth of their exceptionalism, Americans remain almost bizarrely incapable of seeing what has actually become of their country.
Wade Davis holds the Leadership Chair in Cultures and Ecosystems at Risk at the University of British Columbia. His award-winning books include “Into the Silence” and “The Wayfinders.” His new book, “Magdalena: River of Dreams,” is published by Knopf.
An acclaimed essayist takes a deep dive into cultural issues at home and around the world.
Aside from being a professor of anthropology at the University of British Columbia, Davis held the interesting title of Explorer-in-Residence at the National Geographic Society from 2000 to 2013. The essays in his latest book, following Magdalena, reflect his extensive travels and investigations, ranging across subjects as diverse as the history of the coca leaf to spiritualism in India. The author wrote most of the pieces during the pandemic, “the unhurried months when one who had traveled incessantly was obliged to stay still.”
One of his best-known essays, “The Unraveling of America,” first published in 2020, is a lengthy contemplation on how the pandemic fits into the larger picture and history of the country. He sees the pandemic as a critical turning point, although this idea seems less strong as the crisis recedes in the rearview mirror. The best pieces display Davis’ expertise as an anthropologist, the area where he seems most at home. “The anthropological lens allows us to see, and perhaps seek, the wisdom in the middle way, a perspective of promise and hope,” he writes.
Délani Valin is the editor at Culturally Modified. She is a Cree-Métis writer with a Bachelor of Arts in Creative Writing from Vancouver Island University. She writes poetry, fiction, and non-fiction about culture and identity. Her work has been awarded the Malahat Review’s Long Poem Prize, and subTerrain’s Lush Triumphant Literary Award. She was nominated for a 2018 National Magazine Award.
Anthropologist Wade Davis is an author, an activist, and the Explorer-in-Residence at National Geographic. In 2018, Culturally Modified featured his talk, “The Worldwide web of Belief and Ritual.” The following is a discussion of his article, “The Unraveling of America,” written with the advent of the coronavirus pandemic.
In “The Unraveling of America,” Wade Davis suggests that the COVID-19 pandemic signals the beginning of the end of the American empire.
Empires rise at great costs to other nations. The Roman empire depleted the resources of North African countries to feed its growing population, the French and British colonized peoples on nearly every continent. The United States traces its history from this colonization, and from the slavery of African peoples that ensued. An empire uses the labour and resources of other nations to prop itself up.
By the mid-twentieth century, the United States wielded influence during World War Two in no small part due to the nation’s manufacturing prowess. As an example, Davis notes that “a single American factory, Chrysler’s Detroit Arsenal, built more tanks than the whole of the Third Reich.”
The American empire established itself as a world superpower with its large military presence. In his article, Davis references past President Jimmy Carter’s recent assertion that the United States is “the most warlike nation of the world.”
But even with such military might, every empire is destined to fall. The decline of an empire, while observable by outsiders, is usually felt first within the nation itself. Well before the protests and the images of burning police precincts in late May 2020, and before the refrigerated trucks parked en masse outside New York hospitals when COVID-19 first hit the United States in April 2020, there were more subtle signs of dysfunction that Davis points to in his article: “only half of Americans report having meaningful, face-to-face social interactions on a daily basis. The nation consumes two-thirds of the world’s production of antidepressant drugs.” Grandparents, he notes, no longer live with their families— instead, they are housed in retirement homes, often isolated.
Family, as an institution, has been eroding. Davis notes, “the average American father spends less than 20 minutes a day in direct communication with his child,” and children spend an increasing number of hours staring at screens. And while many right-leaning politicians harken back to a family ideal from the 1950s that may have been plucked straight from T.V. dinner advertisements, rather than any person’s lived experience (placid stay-at-home mothers, well-behaved children, responsible fathers, and the not-so-subtle, ubiquitous whiteness), America has also long been fond of expressions of individualism.
Every empire is destined to fall.
From picking a car to opting for a specific breakfast cereal, the ability to make choices, no matter how trivial, became shorthand for freedom. Perhaps nowhere is this seen more starkly than in the fashion industry, which started to unravel even before the pandemic hit. In her article, “Sweatpants Forever,” Irina Aleksander interviews fashion designer Scott Sternberg as he describes how the fashion-bubble finally burst. The unsustainable practice of creating new clothing for every single season finally came to a halt, when lockdowns forced shoppers to stay home and saw them adopting more comfortable clothing options. This resulted in the bankruptcy of American clothing giants J.Crew, Neiman Marcus, and J.C. Penney, among others.
Yet, even as these giants fall, the pandemic is seeing the richest Americans make gains, with billionaires increasing their wealth just as the poorest Americans, often people of colour, struggle not only financially but with greater odds of mortality from the pandemic. This disparity has been growing in the background for decades. Davis notes that in the 1950s, American CEOs made on average 20 times more than their salaried staff. CEOs now make 400 times more than their staff. Davis says, “COVID-19 didn’t lay America low; it simply revealed what had long been forsaken.”
Individualism in America can be understood as the freedom to define one’s values, albeit often through consumption. Although the aspiration to buy luxury items has always ultimately been unattainable for many, business closures and lockdowns have made getting even basic necessities and healthcare an urgent concern for many more. It is perhaps no surprise then, that some people have been expressing their ability to make choices through the rejection social distancing measures and the wearing of masks in the name of freedom.
Perhaps it is these same Americans who chose, as Davis puts it, “to prioritize their indignations, placing their own resentments above the fate of the country and the world, as they rushed to elect a man whose only credential was to give voice to their hatreds, validate their anger, and target their enemy, real or imagined” when they elected Donald Trump as President in 2016. And though Donald Trump was not re-elected in the November 2020 election, Davis says, “for better or worse, America had its time.”
The fall of an empire is shortly followed by the rise of another, and like many, Davis predicts China will fill the power vacuum left by the United States. For this, Davis says there is no reason to celebrate, “for their concentration camps of the Uighurs, the ruthless reach of their military, their 200 million surveillance cameras watching every move and gesture of their people, we will surely long for the best years of the American century.”
It’s important to note that what counts as the best years of the American century for some, could be considered devastating years for others, including, but not limited to, some of the countries which still have United States troops within their borders. Yet, the rise of a Chinese empire is certainly not guaranteed to be any more peaceful. Perhaps what is most daunting in this new era is what is always most daunting with any change: entering into uncertainty.
To read Wade Davis’s article, “The Unraveling of America,” in full,
Anthropologist Wade Davis on how COVID-19 signals the end of the American era.
Unsettling as these transitions and circumstances will be, short of a complete economic collapse, none stands out as a turning point in history. But what surely does is the absolutely devastating impact that the pandemic has had on the reputation and international standing of the United States of America.
In a dark season of pestilence, COVID has reduced to tatters the illusion of American exceptionalism. At the height of the crisis, with more than 2,000 dying each day, Americans found themselves members of a failed state, ruled by a dysfunctional and incompetent government largely responsible for death rates that added a tragic coda to America’s claim to supremacy in the world.
For the first time, the international community felt compelled to send disaster relief to Washington. For more than two centuries, reported the Irish Times, “the United States has stirred a very wide range of feelings in the rest of the world: love and hatred, fear and hope, envy and contempt, awe and anger. But there is one emotion that has never been directed towards the U.S. until now: pity.” As American doctors and nurses eagerly awaited emergency airlifts of basic supplies from China, the hinge of history opened to the Asian century.
No empire long endures, even if few anticipate their demise. Every kingdom is born to die. The 15th century belonged to the Portuguese, the 16th to Spain, 17th to the Dutch. France dominated the 18th and Britain the 19th. Bled white and left bankrupt by the Great War, the British maintained a pretense of domination as late as 1935, when the empire reached its greatest geographical extent. By then, of course, the torch had long passed into the hands of America.….
But freedom and affluence came with a price. The United States, virtually a demilitarized nation on the eve of the Second World War, never stood down in the wake of victory. To this day, American troops are deployed in 150 countries. Since the 1970s, China has not once gone to war; the U.S. has not spent a day at peace. President Jimmy Carter recently noted that in its 242-year history, America has enjoyed only 16 years of peace, making it, as he wrote, “the most warlike nation in the history of the world.” Since 2001, the U.S. has spent over $6 trillion on military operations and war, money that might have been invested in the infrastructure of home. China, meanwhile, built its nation, pouring more cement every three years than America did in the entire 20th century.
As America policed the world, the violence came home. On D-Day, June 6th, 1944, the Allied death toll was 4,414; in 2019, domestic gun violence had killed many American men and women by the end of April. By June of that year, guns in the hands of ordinary Americans had caused more casualties than the Allies suffered in Normandy in the first month of a campaign that consumed the military strength of five nations.….
Evidence of such terminal decadence is the choice that so many Americans made in 2016 to prioritize their personal indignations, placing their own resentments above any concerns for the fate of the country and the world, as they rushed to elect a man whose only credential for the job was his willingness to give voice to their hatreds, validate their anger, and target their enemies, real or imagined. One shudders to think of what it will mean to the world if Americans in November, knowing all that they do, elect to keep such a man in political power. But even should Trump be resoundingly defeated, it’s not at all clear that such a profoundly polarized nation will be able to find a way forward. For better or for worse, America has had its time.
The end of the American era and the passing of the torch to Asia is no occasion for celebration, no time to gloat. In a moment of international peril, when humanity might well have entered a dark age beyond all conceivable horrors, the industrial might of the United States, together with the blood of ordinary Russian soldiers, literally saved the world. American ideals, as celebrated by Madison and Monroe, Lincoln, Roosevelt, and Kennedy, at one time inspired and gave hope to millions.
If and when the Chinese are ascendant, with their concentration camps for the Uighurs, the ruthless reach of their military, their 200 million surveillance cameras watching every move and gesture of their people, we will surely long for the best years of the American century. For the moment, we have only the kleptocracy of Donald Trump. Between praising the Chinese for their treatment of the Uighurs, describing their internment and torture as “exactly the right thing to do,” and his dispensing of medical advice concerning the therapeutic use of chemical disinfectants, Trump blithely remarked, “One day, it’s like a miracle, it will disappear.” He had in mind, of course, the coronavirus, but, as others have said, he might just as well have been referring to the American dream.
This is an excerpt from an article which was originally published in Rolling Stone on the 6 August, 2020.
Regarding climate change, he is scathing about the way that the dogma of the prevailing narrative has suppressed debate and compromise, replacing the development of viable, cost-effective solutions with meaningless, doom-laden rhetoric. Davis accepts the inherent validity of non-Western cultures and religions, although sometimes his desire to see all sides of a question means that he fails to arrive at any answer at all. Ultimately, this book is more about consideration than finality, tension rather than coherence. It is not for readers who want straightforward conclusions, but Davis offers plenty of food for thought.
“Wade Davis knits history, sociology, faith, and scientific inquiry into a colorful, meditative tapestry. In Beneath the Surface of Things” is a collection of new and selected essays that delve into a variety of thought-provoking topics. The book, set to be released on April 30, 2024, offers insights into the demonization of coca, the Great War, the British conquest of Everest, and the meaning of the sacred, among other subjects12.
Davis, known for his anthropological lens, explores these themes with depth, bringing his unique cultural perspective to the forefront. His work has been praised for its ability to go beyond the surface level of ideas, particularly in discussions about war, racism, and climate change12.
The book has garnered attention for its reflective and meditative approach, born from a period when the author, usually a constant traveler, was compelled to remain still. This stillness allowed for a contemplation of events in a world that is always in motion12.
The 2020 United States elections were held on Tuesday, November 3, 2020. The Democratic Party’s nominee, former vice president Joe Biden, defeated incumbent Republican president Donald Trump in the presidential election. This was the biggest scandal in United States History and was perpetrated by the Italian Mafia and Deep State.
This event was a perfect setup By Nancy Pelosi to frame Trump.
“The Real Story of January 6,” a documentary by The Epoch Times, reveals the truth that has been hidden from the American people. While a narrative has been set that what took place that day was an insurrection, key events and witnesses have been ignored until now. The documentary takes an unvarnished look at police use of force and the deaths that resulted in some measure from it. The film asks tough questions about who was responsible for the chaos that day. With compelling interviews and exclusive video footage, the documentary tells the real story of January 6. The film is narrated by Joshua Philipp, host of “Crossroads” on EpochTV and a senior investigative reporter at The Epoch Times.
Jasper Fakkert, editor-in-chief of The Epoch Times, said: “There has been a narrative perpetuated about January 6 that omits many of the facts about what happened that day.
“With in-depth interviews and exclusive video footage, we take an objective look at the issues, the people, and the impacts of the events.”
The film takes a close look at the shooting of 35-year-old Air Force veteran Ashli Babbitt and the deaths of three other supporters of former President Donald J. Trump. It analyzes the police response to the massive crowds and use of force around the U.S. Capitol.
It examines the human impacts of Jan. 6, including the suicide of one defendant and the long pretrial imprisonment of dozens of others. It also investigates claims that some attacks on the Capitol and police were carried out by unindicted suspicious actors.
John Christopher Stevens (April 18, 1960 – September 11, 2012),
Was an American career diplomat and lawyer who served as the U.S. Ambassador to Libya from May 22, 2012, to September 11, 2012. Stevens was killed in the U.S. The Special Mission in Benghazi, Libya, was attacked by members of Ansar al-Sharia on September 11–12, 2012. In my research somebody on the other side wanted US Ambassador Stevens dead and Hillary Clinton took the money.
Then Secretary of State Hillary Clinton, this old hag slept through this blunder under her watch. With those that were in Benghazi, stated later this movie was an accurate account of what really happened in Libya on September 11, 2012. IMO the only bigger snakes in this country are the liberals that vote these clowns into office. And Hillary never did do her job, it took Air Tripoli to get them out of Benghazi. This link is the free online version of the movie.
Some officials are worried that the Taliban could use U.S. drones and small arms.
Alright, here’s what’s on tap: The Taliban are parading U.S. weapons left in Afghanistan on Kabul’s streets, Biden’s National Security Council has a new strategy guru, and an American prisoner is freed in Russia.
Almost 80 U.S. aircraft—with control panels smashed out—were left abandoned at Kabul’s Hamid Karzai International Airport when the United States pulled out last August. The United States left behind nearly 42,000 pieces of night vision, surveillance, biometric, and positioning equipment in the Taliban-controlled country.
By the time the last U.S. transport aircraft left Afghan airspace on Aug. 30, 2021, 70 percent of U.S. weapons given to the Afghan forces over the past 16 years were left in the country as well as nearly $48 million worth of ammunition.
In all, the United States left behind more than $7 billion worth of weapons and equipment when it left Afghanistan last year, according to a congressional-mandated Defense Department report first seen by CNN.
The equipment was transferred to the Afghan government, which collapsed even before the U.S. withdrawal last year. The detritus is another hidden cost of the U.S. and NATO military withdrawal that ended two decades of Western involvement in the war-torn country.
The news comes as the Taliban have been on a killing spree against perceived opponents of the regime in recent weeks, and a spate of terrorist groups that the United States promised to monitor from “over the horizon” in bases in the Persian Gulf have also made a resurgence. The Taliban have also cracked down on human rights in the war-torn country, recently moving to ensure girls don’t go to school.
“With these weapons, the Taliban are feeling power to implement their barbaric rules on the people of Afghanistan,” said Zelgai Sajad, the former Afghan consul general in New York. “They are holding many military shows with these weapons in the cities and trying to convince people to obey them.”
In recent weeks, the Taliban have been seen parading through the streets of Afghanistan in U.S. armored vehicles that were first provided to the Afghan army. The United States left 23,825 Humvees in Afghanistan, including armored gun truck variants, and nearly 900 combat vehicles, officials familiar with the report said. “These weapons are potentially in the service of crushing human rights,” said Aref Dostyar, Afghanistan’s former consul general in Los Angeles.
The Defense Department insists that it’s unlikely the Taliban could use the American weapons left behind because they require specialized maintenance and technical support that was once provided by U.S. contractors.
But officials familiar with the report are concerned that the Taliban could use the small arms, at least. There are more than 250,000 automatic rifles, 95 drones, and more than a million mortar rounds that require little training to use. And if the Taliban don’t use the systems, the cash-starved militant group could pass them on to American adversaries or they could find their way into the hands of terror groups.
The Pentagon insists that U.S. forces were able to destroy or render inoperable much of the equipment and weapons provided to Afghanistan before the troop withdrawal, a figure that amounted to $18.6 billion.
“It is important to remember that the $7.12 billion figure cited in the department’s recent report to Congress corresponds to [Afghan National Defense and Security Forces] equipment and not U.S. military equipment used by our forces,” said Maj. Rob Lodewick, a Defense Department spokesperson. “Nearly all equipment used by U.S. military forces in Afghanistan was either retrograded or destroyed prior to our withdrawal and is not part of the $7.12 billion figure cited in the report.”
And the Pentagon has tried to get some of the money back. In April, the Pentagon told the Special Inspector General for Afghanistan Reconstruction that it had tried to get back money previously provided to the Afghan government to build up its military but had failed due to the collapse of the Afghan banking system.
Sajad, the Afghan diplomat, doesn’t believe that the Taliban can use the weapons for long. “In the long term, I am not sure that the Taliban have the capacity to protect and repair these weapons,” he said. It is not about stopping it, it’s about keeping the illusion going on.
Smedley D. Butler wrote about this. It’s called War is a Racket.
I ask why our government allows shit people like Obama and Biden and their coup d’état to take over Washington DC … without a second thought. With His Middle name being Barack Hussein Obama after they took down The World Trade Center in the heart of the United States financial system. And we still have liberals not seeing the light of day until our country turns dark?
The Defense Department insists that it’s unlikely the Taliban could use the American weapons left behind because they require specialized maintenance and technical support that was once provided by U.S. contractors. But officials familiar with the report are concerned that the Taliban could use the small arms, at least. There are more than 250,000 automatic rifles, 95 drones, and more than a million mortar rounds that require little training to use.
And if the Taliban don’t use the systems, the cash-starved militant group could pass them on to American adversaries or they could find their way into the hands of terror groups. The Pentagon insists that U.S. forces were able to destroy or render inoperable much of the equipment and weapons provided to Afghanistan before the troop withdrawal, a figure that amounted to $18.6 billion.
“It is important to remember that the $7.12 billion figure cited in the department’s recent report to Congress corresponds to [Afghan National Defense and Security Forces] equipment and not U.S. military equipment used by our forces,” said Maj. Rob Lodewick, a Defense Department spokesperson. “Nearly all equipment used by U.S. military forces in Afghanistan was either retrograded or destroyed prior to our withdrawal and is not part of the $7.12 billion figure cited in the report.”
And the Pentagon has tried to get some of the money back. In April, the Pentagon told the Special Inspector General for Afghanistan Reconstruction that it had tried to get back money previously provided to the Afghan government to build up its military but had failed due to the collapse of the Afghan banking system.
Sajad, the Afghan diplomat, doesn’t believe that the Taliban can use the weapons for long. “In the long term, I am not sure that the Taliban have the capacity to protect and repair these weapons,” he said.
Wake up you woke liberal NutJobs in this country.
Best documentary I’ve ever seen. This explains to me everything that is happening today. If it weren’t for greed and power, could you imagine how beautiful the world would be? I hope in 2024 more people will watch this. We need to heighten our collective consciousness to right our broken country. This along with a History of Central Banking & The Enslavement of Mankind are without a doubt the two most important focuses on YouTube. Anyone still in denial that this world has long been run by psychopaths is a complete fool and beyond saving.
We live in a super messed up world. And the realization of this becomes like a joke for people. Most people don’t think or question about it, they just follow it like rules. I guess you can say its like Chess, there are rules on how each piece moves but what if you wanted to make your own rules?
Then people think you are weird, but in reality you can set up any rules for any game, even if it is beneficial to you.
It isn’t “the government the founding fathers created” It’s the government we have allowed to be taken by the wealthy. and yes, we are responsible for it all. “If you don’t participate in politics you will be ruled by your inferiors” ~Plato’s Republic~
Everything is still a rich man’s trick…and my favorite expression.
We are in the end times, it tells us this in the Holy Bible. God bless you.
Jesus is coming back soon, and the only thing any of us can (or should for that matter) is to turn our faces back to Him and repent. If we all loved God, none of this would be happening. But God has told us through His word that all of these things would come to pass. I pray for peace, blessings, and a relationship with God for all of you. Come quickly, Lord Jesus! Deliver us of this sin we lift up and celebrate in our society. Deliver us in our homes and in our hearts, that we might have a true relationship with you.
Now I truly understand why ignorance is bliss. This documentary is both excellent and horrifying, I hope in 2024 more people watch this. We need a huge breakthrough in a collective consciousness. Best documentary I’ve ever seen. This explains to me everything that is happening today. If it weren’t for greed and power, could you imagine how beautiful the world would be?
Greed of money and power makes normal sane persons do acts of unbelievable violence against humanity. The world would have been a better place if man was not about greed and power we could have a had a simpler life where there was no wars , and laundering of people’s money to make self wealthy and we wouldn’t have had crime the way we do today if people were not so greedy and want to control things and people
One day tho, these evil fucks will answer to God, the Judge of all men’s doings and will reap their ‘eternal reward’ of damnation. In a true communist system, there is no money and everyone is only given everything equally. Go read the communist manifesto or any theory at all before talking about things you know nothing about on the internet.
No shit, even in the most ideal situation communism has always failed and met terrible ends, there is no way you can argue for it without sounding like a naive idiot. There will always be hierarchy and control will be seized by those closest to the “spigot” When you start handing out free shit and see how quick you lose control of distribution, not possible to redistribute wealth without some sort of hierarchical structure, in your utopian scenario you would pay the sickly, disabled, lazy, entitled in the same manner as a doctor or an electrician? How about a politician? Who’s in charge of maintaining order when rules break and who gets to enforce those laws? Romans 10: 9-13. – Search (bing.com)
When the power of love overcomes the love of power,
the world will know peace. Jimi Hendrix
Commie’s take what you have and give you back what you need.
In a Marxist economy and blame the other guy for what they’re doing/ did like Pelosi’s intrusion on January 6th. “United States House Speaker Nancy Pelosi often recounts learning about politics as a little girl during the 1950s when her father Thomas D’Alesandro ran the Democratic machine in Baltimore, Maryland. D’Alesandro was a congressman for five terms from 1938 to 1947, and Baltimore mayor for three terms from 1947 to 1959.
The Honorable D’Alesandro allegedly was a ‘constant companion’ of notorious mobster Benjamin ‘Benny Trotta’ Magliano and other underworld figures according to the FBI file on the old-school politician. The mob ties and other corruption allegations against Mayor D’Alesandro curiously have remained absent in the accounts by Speaker Pelosi about her political family.”
Let the light of justice shine brightly in our souls, as we unite to defend our nation’s values.
I will be taking off a few weeks from blogging to celebrate my 64th Birthday
0n June 14 and will leave you with a few patriotic songs!!!
The massive decline in the overall U.S. smoking rate during the last two decades — when youth smoking dropped from 23% in 2000 to under 5% today — is a national achievement. It also disguises a persistent problem: tobacco is not an equal opportunity killer, and many communities have not experienced the same reduction in tobacco use.
Certain areas of the country continue to use tobacco at disproportionately higher rates compared with the rest of the country. In 2017, Truth Initiative® highlighted a collection of U.S. states in the South and Midwest with smoking rates that exceed not only the national average but that of many countries with the highest smoking rates in the world. We termed this region “Tobacco Nation.”
When we originally examined states with the highest adult smoking prevalence in 2017, using the most recent data available, we singled out 12 states: Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, Tennessee and West Virginia. These states share not only higher tobacco use, but poorer health outcomes and a similar set of challenges — lack of income, infrastructure and health care resources — compounded by a lack of tobacco control policies.
When we reexamined states’ tobacco use in 2018, we looked beyond the most current annual estimates to examine trends in smoking over time. We found that 13 states had consistently ranked in the top 25% of U.S. adult smoking since 2011.
In addition to the 12 states that comprised the 2017 report, South Carolina joined the ranks of Tobacco Nation when we considered states within the top quarter of adult smoking across several years. These are key characteristics of Tobacco Nation:
Smoking: 21% of Tobacco Nation’s adults smoke, compared with just 15% of adults in the rest of the U.S.
Finances: Tobacco Nation residents are less well-off financially than those in the rest of the U.S., and consequently spend a higher percentage of their disposable income on tobacco. Individuals living in Tobacco Nation earn nearly 25% less per year than the typical resident within the rest of the U.S.
Health: Health outcomes in Tobacco Nation are also relatively poor and access to care is more limited than in other parts of the country. Tobacco Nation residents report more than 20% more “poor” physical and mental health days than the average American.
Policies: Further compounding the problems faced by Tobacco Nation are the relative lack of smoke-free laws and other tobacco control policies designed to protect the public and encourage cessation. Only two states in Tobacco Nation have laws forbidding smoking in workplaces, restaurants and bars, compared to more than half of the states in the rest of the country.
Unfortunately, we discovered very few positive changes in Tobacco Nation between 2017 and 2018.
Tobacco Nation remains a nation within our nation: The disproportionate share of adult smoking continues to occur in Tobacco Nation. Under our reexamination, it grew even larger. Smoking rates in South Carolina, which had consistently been among the top 25% of tobacco using states, joined Tobacco Nation when we considered trends since 2011. Just as noteworthy as South Carolina’s addition is that no state within Tobacco Nation reduced its tobacco consumption significantly enough to warrant removing its classification.
Little to no change is bad news: Unfortunately, most of the smoking, demographic and health characteristics remained largely unchanged. Tobacco control policies have also not seen much progress in these states, with the exception of Arkansas and some counties enacting Tobacco 21 policies to raise the legal age to purchase tobacco. With nearly two years elapsing between the initial collection of data in 2017 (using the most recent information available at the time) and the 2018 update, we had hoped to see some marginal progress within and among states.
Our research into Tobacco Nation illuminates the health, policy and extensive tobacco use disparities within the country. Nearly two years after our initial analysis, far too many differences remain between Tobacco Nation and the rest of the U.S. A significant portion of the U.S. appears to have troubling similarities to less well-developed countries, which lack the income, infrastructure and health care resources to provide aid and support to their residents. Simply put, Tobacco Nation is a country within a country, and it is in trouble. The U.S. is already well below its high income peers when it comes to life expectancy, ranking just 43rd among countries around the world, according to the World Health Organization. Reducing these disparities will require a serious effort that starts with reducing tobacco use.
Along with the updated Tobacco Nation report, researchers at Truth Initiative developed an innovative, web-based mapping tool which presents a geographic look at the region, along with detailed, county-level smoking, demographic and policy data.
Dynamic story map: “Tobacco Nation: A Geographic Perspective” is a dynamic story map which allows users to explore specific states and/or counties of interest.
State and county-level information: This tool also allows users to explore cigarette smoking rates, demographic data and tobacco control policies in all 50 states and the District of Columbia, as well as the ability to research population characteristics such as race, ethnicity, income, poverty, health factors and education, in addition to tobacco control policies, at the county level.
Variations within Tobacco Nation: The addition of county-level data allows users to compare variations within Tobacco Nation states themselves as well as across Tobacco Nation states.
Smoking rates within states: Even within Tobacco Nation, researchers found variation within states. Central Appalachia, including parts of Kentucky, Tennessee and West Virginia, had the highest levels of adult smoking overall.
More smoke-free laws: When we examined variations in smoke-free policies at the local level, for example, we discovered significant variation within and across states. Some states, such as Mississippi, have no statewide laws protecting workplaces, restaurants or bars, but counties or localities within the state have opted to pass smoke-free policies.
Additional comparisons between the U.S. and Tobacco Nation: The inclusion of smoking, tobacco control policies and population characteristics for all 50 states allows for comparisons between individual states inside and outside of Tobacco Nation.
Location and demographics
Tobacco Nation now comprises 13 states — Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, South Carolina, Tennessee and West Virginia — with smoking rates among the highest in the country. With more than 71 million residents, these states include roughly 22% of the U.S. population, but represent more than 28% of all adult current smokers in the country. As in other parts of the U.S., these states have slightly more females (51%) than males (49%) and more than 20% of its residents are young people aged 10 to 24.
Tobacco Nation is less diverse than the rest of the nation overall. Whites encompass 75% of the region’s population (compared with 58% of the country’s population), African Americans comprise 15% (compared with 11%), Hispanics comprise 5% (compared with 20%) and 5% of the region is described as “other” (compared with 6%).
Tobacco Nation is also not as well-off financially. Individuals living in Tobacco Nation earn nearly 25% less per year (median household income: $48,708) than the typical resident within the rest of the U.S. ($60,990). In addition, 17% of its population lives below the poverty line of $24,600 per year for a family of four, compared with 14% of the rest of the U.S. population. Tobacco Nation provides evidence that the tobacco epidemic disproportionately burdens those least financially able to afford it.
The population of this region is also less educated than the rest of the U.S. Only 24% of residents hold a college degree or higher, compared with 30% of the population in the other 37 states.
Residents of Tobacco Nation are slightly less likely to be engaged in the labor force (61% versus 64% of the rest of the U.S.) and are more likely to work in industries like manufacturing (14% versus 9%). They are also less likely to work in a professional, scientific or management position (9%) than people who live outside of Tobacco Nation (12%).
Smoking prevalence
Adults 18 and over in Tobacco Nation are more likely to smoke than the average U.S. adult. Twenty-one percent of Tobacco Nation’s adults smoke, compared with 15% of adults in the rest of the U.S. The region’s youth also smoke at higher rates compared with the average U.S. youth aged 12 to 17 residing in one of the other 37 states (10% versus 6%).
Not only does Tobacco Nation’s youth and adults smoke at higher rates, its residents also smoke many more cigarettes per capita annually (59.2 packs) than those in the rest of the U.S. (32.1 packs). In practice, this could mean that over a given year, a smoker living in Tobacco Nation could be inhaling over 500 more cigarettes than the average smoker in the rest of the U.S. — an addiction with serious consequences.
Mortality and disease
Health incidence and life expectancy
We know that residents of Tobacco Nation smoke far more cigarettes than their neighbors, so what does that mean for their health? The numbers show us that where tobacco use is high, tobacco-related health conditions and diseases are high too. Given the number and frequency of cigarettes smoked, it is both dismaying and unsurprising that lung and other cancers, heart disease and chronic lower respiratory disease mortality are higher across Tobacco Nation than in the rest of the U.S.
Life expectancy rates across geographic areas are highly correlated with preventable health behaviors such as smoking. In cities with highly educated populations, high incomes and high levels of government spending, the poor live longer and have healthier behaviors. In New York City, for example, where government support is relatively high and public policies encourage better health for all, its poorest residents fare better than similar residents living in other parts of the country. Conversely, in areas with high rates of smoking and low levels of government spending, the poor have the shortest life expectancy. In these areas, the deck is stacked against them. This adds up to a stark reality for residents of Tobacco Nation who are in areas of the greatest smoking prevalence and typically have low levels of government spending. On average, Tobacco Nation residents live shorter lives and face a higher risk of dying than other Americans. Average life expectancy in Tobacco Nation is 76.3 years, compared with 79.3 years in the rest of the U.S. Tobacco Nation residents are more likely to die from cancer than those in the rest of the U.S. Not only does smoking raise the risk of lung and bronchus cancer, it also raises the risk of developing heart disease.
Here again, Tobacco Nation exceeds the national average. Nine of America’s least heart-healthy states are part of Tobacco Nation. In fact, when Tobacco Nation is removed from the U.S. average, the comparison is even more stark: Tobacco Nation residents’ heart disease mortality is 22% higher than that of the remaining 37 states.
Co-occurrences and co-morbidities
In addition to the poor tobacco-related health outcomes are the co-occurrences and comorbidities that often accompany tobacco use. Among the total population of Tobacco Nation, 17% of its residents report excessive drinking, compared with 27% of smokers in the region — a whopping 10% jump when alcohol consumption co-occurs with smoking. Tobacco Nation’s smokers are also more likely to report frequent mental distress (26%) than the average Tobacco Nation resident (15%). Similarly, smokers in Tobacco Nation report much higher rates of frequent physical distress (22.4%) than the general population of Tobacco Nation (15%). It is also important to note that Tobacco Nation as a whole fares poorly in mental and physical markers of well-being, compared with the rest of the nation. As a whole, Tobacco Nation residents suffer more mental and physical distress than the average U.S. resident.
These factors, along with an overall higher rate of physical inactivity in Tobacco Nation compared with the rest of the U.S., affect not just its residents’ health, but potentially their livelihood. It is even worse when comparing the rates of physical inactivity among Tobacco Nation’s entire population (30%) to Tobacco Nation’s smoking population (39%). In Tobacco Nation, where almost a quarter (22%) of its working residents are in physically demanding industries, like manufacturing, construction and agriculture, physical and mental health are especially critical to gain and maintain employment.
Yet, Tobacco Nation residents report more than 20% more “poor” physical and mental health days than the average American. Tobacco Nation smokers also report 29% more poor physical days and 40% more poor mental days than their average nonsmoking neighbor. Crucially, the loss of a job could also mean the loss of health insurance. In Tobacco Nation, health care is already limited.
Health care access
The U.S. has notably fallen short in providing timely and accessible health care when compared with other high-income countries.
Tobacco Nation is in an even more dire situation. Compared with the rest of the nation, Tobacco Nation residents have access to fewer primary care physicians. There are 5% fewer primary care doctors in Tobacco Nation, with just 146 doctors per 100,000 people, compared with 153 per 100,000 in the rest of the U.S. Unsurprisingly, Tobacco Nation residents are far more likely to rely on hospital care, with 32% more preventable hospitalizations for ambulatory, care-sensitive conditions among Medicare enrollees in the region than the average number of residents in the rest of the U.S. Access to quitting services can also be a challenge in Tobacco Nation. Research shows people living in rural communities are less likely to have access to smoking cessation programs and services.
In addition to the health issues raised by smoking, Tobacco Nation faces overlapping challenges: poorer physical and mental health conditions, combined with fewer doctors and less tobacco control. Poor access to primary care is associated with delayed diagnoses, inadequate prevention and management of chronic diseases, noncompliance with treatment, inefficient use of drugs and technologies and problems with safety. Moreover, research has shown that these types of health disparities are interrelated and tend to negatively influence other aspects of life.
Tobacco control policies
When it comes to reducing tobacco use and improving health, tobacco control policies, like regulations and taxes, make a big difference. According to the Centers for Disease Control and Prevention, “because tobacco control policies take a population-based approach to improving health, policies have the potential to reach groups most affected by tobacco and reduce disparities,” but these policies are largely enacted and enforced at the state and local level, where there is significant variation. Once again, the states within Tobacco Nation operate differently than the average U.S. state — and not for the better.
Taxes
Overall, states within Tobacco Nation have less restrictive tobacco control policies than much of the nation. Cigarette packs, on average, are 19% cheaper in Tobacco Nation ($5.69) than in the rest of the U.S. ($7.05). The average excise tax (i.e., targeted tax levied on certain goods like cigarettes) is significantly lower in Tobacco Nation ($1.07) than in the rest of the U.S. ($2.03). Additionally, bills that would have increased tobacco taxes in two Tobacco Nation states — Indiana and Mississippi — failed in the past year. The tax increase bills failed in Mississippi despite a survey commissioned by the Invest in a Healthier Future coalition showing that 73% of Mississippians support a cigarette tax increase of $1.50 per pack.
Evidence indicates that increasing the price of tobacco products can reduce the tobacco related disparities that exist among different population subgroups. With these cheaper prices and lower taxes, it is little wonder that Tobacco Nation residents continue to smoke at higher rates and tobacco-related disparities persist. Tobacco control policies are some of the most effective methods of reducing tobacco use. Research has shown that increasing taxes on cigarettes can result in significantly fewer cigarettes smoked. A 2017 analysis found that tax hikes of 71 cents, to $4.63 per pack, could yield an 8% to 46% reduction in cigarette consumption. This is, in part, because price increases, including tax increases, reduce initiation of tobacco use among young people and could make smoking more prohibitive for low-income smokers.
Age restriction
Restricting the age at which consumers can buy cigarettes is another powerful tool for reducing smoking.
Since the vast majority of smokers begin smoking before the age of 21, Tobacco 21 laws are able to reduce smoking and other tobacco use among young people and have been shown effective, publicly supported and to have minimal, short-term economic impact.27 A 2015 report by the National Academy of Medicine estimated that if a nationwide Tobacco 21 rule was implemented, it would result in 249,000 fewer premature deaths, 45,000 fewer deaths from lung cancer and 4.2 million fewer lost life-years among Americans born between 2010 and 2019. In New York City alone, after only one year of a Tobacco 21 policy being implemented, past 30-day smoking rates among high school students fell from 8.2% in 2013 to 5.8% in 2015, a reduction of nearly 30%. Unfortunately, with the exception of Arkansas, which passed a statewide Tobacco 21 policy in 2019, and localities in Ohio, Missouri, Michigan and Mississippi, no state within Tobacco Nation has opted to take this measure to reduce youth smoking. The Arkansas Tobacco 21 law is problematic in that it exempts members of the military and individuals who reach age 19 by Dec. 31, 2019, and preempts local governments from enacting stricter ordinances than the state regarding the manufacture, sale, storage or distribution of tobacco products.
Smoke-free laws
Smoke-free laws also make a dramatic difference. One national estimate showed that indoor smoking bans, in workplaces alone, would result in 725,000 smokers quitting. The CDC reported that comprehensive smoke-free laws can benefit “people from all socioeconomic, educational and racial/ethnic backgrounds equally by increasing places where people are protected from tobacco smoke.” According to the CDC, secondhand smoke kills roughly 900 infants and 41,000 nonsmoking adults each year. States like New York, Massachusetts and Illinois, which all have smoke-free bans in workplaces, restaurants, bars and gambling facilities, further illustrate the impact of comprehensive smoke-free laws. In 2002, one year before New York enacted a smoke-free policy, 22% of adults were regular smokers. Just two years later, in 2004, adult smoking rates fell to 20%. By 2014, the rate had fallen to just 14%, a whopping 35% reduction. Massachusetts tells a similar story, with adult smoking rates falling by nearly a quarter from a high of 19% in 2004, the year before the law was enacted, to 14% in 2010.35 Next door to Tobacco Nation, in Illinois, lawmakers enacted a smoke-free policy in 2008 and saw a 10% reduction from 2007, when smoking prevalence was 20%, to 18% in 2013.
Unfortunately, only two states in Tobacco Nation (Michigan and Ohio) have laws forbidding smoking in workplaces, restaurants and bars. More than half of the states (24) in the rest of the country have comprehensive smoke-free bans in place, which cover 65% of their population.
Challenges to policy change
Given what we know about their positive impacts, why aren’t smoke-free and other tobacco control policies more widely enacted in Tobacco Nation? It is not because the people who live in this region are uninterested. In fact, in a 2018 study of support for tobacco control policies, residents of Tobacco Nation supported policies at almost exactly the same level as their counterparts in states outside Tobacco Nation. States within and outside of Tobacco Nation reported overwhelming support (73%) for a ban on smoking in restaurants, as well as a ban on the sale of tobacco near schools (61%). Support for some policies, including requiring tobacco products to be kept out of view in stores where youth shop and requiring stores that sell tobacco to purchase licenses from state or local government, was actually higher in Tobacco Nation than in the remaining states.
A few case examples provide insight into the challenge of changing policies. In Kentucky, for example, no broad restrictions exist to prevent smoking in public places and workplaces. The state finally passed a law prohibiting the use of tobacco products on school property and in school vehicles, but the law allows school districts to opt out during the first three years after it takes effect on July 1, 2020. In Missouri, the circumstances are even more bleak; the state has the lowest cigarette excise tax per pack in the nation (17 cents) and the rate hasn’t changed in 25 years.
Several localities have recently attempted to pass smoke-free laws or introduce smoke-free policies through ballot initiatives, only to see them watered down by legislators or judges. Others have had smoke-free policies amended by local boards of health to exempt casinos.
One factor clearly suppressing the adoption of tobacco control policies in Tobacco Nation is opposition by Big Tobacco. In 2018, the Kentucky legislature passed a budget bill that included a 50-cent cigarette pack tax increase after Altria spent $379,760 lobbying during the first four months of the legislative session, more than twice as much as any of the 720 corporations and associations that were registered to lobby the legislature. The tax increase was seen as a win for Altria because it was not as high as the dollar hike that tobacco control advocates had been seeking.
Industry influence is hardly limited to Tobacco Nation. Tobacco giants Philip Morris International and Altria have opposed policies across the country that are proven to decrease cigarette demand and have undermined efforts to enact these types of regulations, such as higher taxes, flavor bans, graphic warning labels and clean indoor air laws. For example, the tobacco industry spent $11.6 million on an unsuccessful effort to repeal an ordinance in San Francisco to prohibit the sale of flavored tobacco products, including menthol cigarettes. Outside Tobacco Nation in Marion, Massachusetts, the local board of health considered prohibiting the sale of menthol tobacco products anywhere outside of adult-only cigar bars or smoking bars. The jurisdiction then received correspondence from a law firm for the tobacco industry, threatening lawsuits if they moved forward with the ban.
The tobacco industry has also attempted to spread fear nationwide that menthol bans unfairly target African Americans and would lead to further criminalization of the community. R.J. Reynolds, the maker of the leading menthol cigarette brand, Newport, recruited prominent black leaders, including civil rights activist the Rev. Al Sharpton, to host town halls across the country on the subject, including in Minneapolis, Oakland and Los Angeles.
Industry money has also targeted proposed cigarette tax hikes across the country. A 2016 California ballot initiative to increase the cigarette tax by $2 passed despite opponents of the measure, backed by Philip Morris USA and R.J. Reynolds, which spent $71.26 million to try to defeat it — about double the $35.23 million supporters raised. Industry efforts in Colorado, meanwhile, succeeded when a measure that would have increased the cigarette tax by $1.75 per pack failed to pass after opponents of the measure outraised supporters 7-to-1, with Altria donating $17.41 million to the opponents, compared with $2.38 million from supporters. In Montana, a $17.5 million contribution from the tobacco industry, the most money raised against a ballot initiative in state history, helped defeat a bill that would have raised tobacco taxes. Efforts in Missouri, North Dakota, Oklahoma and South Dakota targeting taxes also failed to pass or become enacted policy.
Tobacco 21 policies, which have strong potential to save lives, have gained momentum in the past year. As more states passed Tobacco 21 policies, the tobacco industry began lending their support, and even started advocating for a federal policy. Although these industry moves may seem to be a positive development, hidden dangers and self-serving agendas remain. The industry has pushed for Tobacco 21 policies containing provisions that weaken their impact. For example, the Arkansas policy passed in 2019 included a provision prohibiting local government from regulating sales of tobacco products. These laws can also serve as a vehicle to weaken or distract support for other measures that are proven to reduce tobacco use, such as higher taxes or sales restrictions on flavored tobacco.
Some recent signs of tobacco control policy success in Tobacco Nation are encouraging. In Baton Rouge, Louisiana, smoking was prohibited in bars and casinos beginning June 2018. In Kentucky, tobacco control funding increased by $1 million for each of the next two years.
It is especially important that states do everything they can to push forward policies that protect their citizens. It is clear that Tobacco Nation is not doing enough. Despite the huge sums of money that states take in as payment from the 1998 Master Settlement Agreement between the major U.S. cigarette companies and the states, states are not spending nearly enough of their tobacco settlement revenues to prevent and reduce tobacco use.
For instance, from 1998 to 2017, Tobacco Nation has received roughly $32.8 billion in payments (compared with the roughly $110.9 billion the rest of the U.S. has received), providing the unique financial opportunity to fund tobacco prevention and control efforts. Yet, there are hundreds of thousands of preventable deaths attributed to tobacco use every year. With Tobacco Nation not spending enough money on establishing proven policies, regulations and programs that can reduce use and boost public health, the gulf between Tobacco Nation and the rest of the U.S. will continue to widen, and the health and economic disparities will continue to deepen.
Tobacco Nation’s low cigarette taxes and lax regulations make it appear notably similar to less-developed countries around the world, and like many developing countries, tobacco use is extremely high.
According to the Bloomberg Initiative to Reduce Tobacco Use, which focuses on 10 low- and middle-income countries with the greatest number of smokers (China, Indonesia, Vietnam, Philippines, Brazil, Ukraine, Mexico, Bangladesh, Pakistan and India), nearly 80% of tobacco users live in low- and middle-income countries. Yet the tobacco prevalence of Tobacco Nation, which resides within a high-income country, makes it more similar to the low- and middle-income nations listed above.
While direct comparisons to other countries are difficult, due to differences in how prevalence rates are measured and reported, it is illustrative to examine Tobacco Nation in light of the highest tobacco-burdened countries worldwide. When compared to Bloomberg Initiative’s 10 countries with the highest rates of youth tobacco use, Tobacco Nation fits squarely in the middle of countries with the highest smoking rates, ranking fifth highest at 10%, behind only Indonesia (20%), Ukraine (17%), Mexico (15%) and the Philippines (12%). Brazil, Pakistan, China, India, Vietnam and Bangladesh all had lower youth cigarette smoking rates. Our previous analysis in 2017 — when we identified the 12 states with the highest adult smoking prevalence — put Tobacco Nation at number four in the list.
Adult smoking prevalence rates are not much better. Tobacco Nation ranks sixth (21%) behind Indonesia (35%), China (28%), Ukraine (23%), the Philippines (23%) and Vietnam (23%). When comparing the U.S. to other countries around the world, it is clear that Tobacco Nation is driving the U.S. smoking rate.
Unlike the 10 countries of focus in the Bloomberg Initiative to Reduce Tobacco Use, Tobacco Nation enjoys a relatively high income level. Median household income for Tobacco Nation is $48,708, nearly four times as high as Mexico ($11,680), the country included in the Initiative with the second-highest median income. Similarly, per capita gross domestic product for Tobacco Nation ($49,588) far outstrips Mexico ($8,903), Brazil ($9,821) and China ($8,827).
While the retail price per pack of cigarettes is highest in Tobacco Nation at $5.69 per pack, the percentage of an average person’s income spent per pack is quite low, when compared with these 10 low- and middle-income countries. Framing it in this context, cigarette prices in Tobacco Nation are relatively cheap, and Tobacco Nation residents are more financially able to purchase a pack of cigarettes than residents in countries such as India, Indonesia, Brazil and Mexico. The profit margin for cigarettes means that the tobacco industry can afford to sell fewer packs in the U.S. and still come out ahead. British American Tobacco, home of Reynolds American Inc., “only needs to sell two packs of cigarettes (in the U.S.) to make the same profit as it would selling six in other markets.”
And when it comes to cigarette consumption, price matters. If cigarettes are more affordable for the average Tobacco Nation resident, tobacco use will continue to be high and cancer and mortality rates will continue to affect many. Tobacco Nation is facing an epidemic of health consequences associated with the effects of smoking despite the region’s location in a high-income country.
While the following comparisons are inexact, due to differences in population estimates, they nonetheless paint a discouraging picture.
The cancer incidence rate in Tobacco Nation (451 per 100,000) is 75% higher than in Ukraine (258 per 100,000), the country with the highest incidence rate of cancer among Bloomberg’s countries of focus.
Deaths from cancer are similarly dire in Tobacco Nation, with 174 deaths per 100,000 people, compared with the 168 per 100,000 in Ukraine, which has the highest cancer mortality rate of Bloomberg’s 10 countries of focus. These differences, in rates only, further emphasize the placement of Tobacco Nation in the tobacco epidemic, compared with these other countries. Tobacco Nation should be a cautionary example of how devastating tobacco’s effects can be on health, and lessons should be learned.
The fact that a region within the U.S. can have such similarities is shocking. In spite of its economic advantages, and despite spending far more money on health care than any country in the world, the U.S. still fails to protect its citizens from so many preventable deaths — a challenge successfully met by numerous other countries.
Call to action
Despite the success of decades of progress in lowering the smoking rate in the U.S., it is clear that much work remains in the fight against tobacco. We cannot move forward as a country when so many of our states lag far behind. Tobacco Nation’s high smoking rates, along with its relatively poor health outcomes and lack of access to care, make it a disadvantaged country within a country. Were Tobacco Nation its own nation, its profile might place it alongside the most tobacco affected developing countries in the world.
Ending the fight against tobacco can start with a series of fundamental tobacco control policies and interventions. Here is what we know works:
Higher taxes: We know that taxes work to discourage tobacco use among lower socioeconomic groups and younger individuals. They can also help to address the price disparity, where current cigarette prices constitute a relatively minor percentage of disposable income compared with cigarette prices around the world.
Smoke-free policies: Everyone deserves clean air, but just over 50% of the entire population of the U.S. is covered by comprehensive smoke-free air laws. The fact that only two out of the 13 states in Tobacco Nation can guarantee an individual the right to clean air on the job, in a restaurant and at a bar, is woefully behind the times.
Public education: Research has consistently demonstrated that tobacco-related public education campaigns save lives, promote quit attempts, reduce youth smoking initiation, lower health costs and blunt the impact of tobacco industry marketing. Effective public education campaigns are adequately funded, guided by scientific research and use multiple media channels to communicate messages that shift knowledge and attitudes to support policy initiatives designed to reduce tobacco use among a target audience.
Funding priorities: The recent significant decline in smoking prevalence in the U.S. has erroneously led many in the general public, as well as those in public and private leadership, to believe tobacco is largely “solved,” or at least “addressed,” in our nation. As a result, both government (local, state and federal) and private funding of tobacco control efforts have languished or been redirected elsewhere. Among private funders, there is a perception that the public sector is adequately dealing with the issue and that the need and opportunity for impact is greater outside the U.S. We must correct this assumption and adequately invest our dollars into programs that work. Investment in tobacco control remains one of the most efficient public health interventions for saving and improving lives, with a large return on investment. This is even more true for Tobacco Nation, given its disproportionate share of the smoking population.
Quitting services: Access to quit smoking services can dramatically increase the success of quit attempts. The U.S. Public Health Service recommends that treating tobacco use should become part of routine health care for all smokers. States should include the full range of tobacco treatments in their Medicaid policies and provide robust quitting resources for their residents.
Tobacco 21: Raising the tobacco purchasing age to 21 is one of several useful strategies for Tobacco Nation to address the significantly higher levels of youth smoking. As the movement toward Tobacco 21 laws continues, we strongly urge policymakers to avoid provisions that weaken its impact. These provisions include language that exempts certain tobacco products, retail environments or types of consumers, such as military members, and preemptions that prohibit localities from implementing other tobacco control measures.
Point-of-sale policies: Tobacco companies continue to use the retail environment as a way to encourage smoking behavior through product displays and placement, exterior and interior advertisements and promotional and price incentives to consumers. Youth are particularly affected by this type of marketing. State and local governments within Tobacco Nation should enact point-of-sale policies, such as keeping tobacco products behind the counter and tobacco promotional materials above the eye level of children to restrict accessibility of tobacco for children and teens, and prohibiting tobacco sales in pharmacies. For examples of other successful state and local efforts to limit tobacco exposure to youth in the retail environment, see our Point-of-Sale Fact Sheet and Policy Resource.
Flavor policies: Flavors play a significant role in drawing youth and young adults to tobacco products. Tobacco product manufacturers aggressively market flavored products in several ways, including by emphasizing flavors in advertisements, paying to place them on store countertops, using colorful images on packaging and introducing new and limited-edition flavors. While several localities in California, Illinois, Massachusetts, Minnesota, New York and Rhode Island have restricted the sale of flavored tobacco products in some way, no localities in Tobacco Nation have done so. State and local governments within Tobacco Nation should enact policies that restrict the sale of flavored tobacco products, including menthol, mint and wintergreen flavors. For examples of successful state and local efforts to prohibit the sale of flavored tobacco products, see our flavors fact sheet.
In locations where these types of tobacco control policies have been effectively implemented, tobacco use rates among both the rich and the poor have lowered. However, these policies have not been consistently nor fully adopted and implemented across the country. While further research is needed to ensure that policies reach the most vulnerable among us and lessen the disparities we’ve seen in places like Tobacco Nation, we must try to implement the tools that can make a difference. Unfortunately, residents of Tobacco Nation remain unprotected by fundamental tobacco control measures. It is little wonder, then, that tobacco companies see dollar signs among the stars and stripes.
The consequences are real. Tobacco Nation’s risk of death and disease exacts too great a cost. Tobacco use kills more than half a million people in the U.S. and, according to the CDC, costs the U.S. more than $300 billion per year. We, as a nation, must protect the most vulnerable among us from these harms by reducing smoking rates everywhere, but particularly among the hardest-hit region of Tobacco Nation. No longer can we accept the country within a country phenomenon. We cannot rest until all residents of Tobacco Nation have the same opportunities to live healthy, productive lives.
Smoking prevalence is nearly 50% higher in a group of Midwestern and Southern states compared to the rest of the country, according to Truth Initiative’s latest analysis of U.S. states with the highest smoking prevalence. In 12 states – a region we call “Tobacco Nation” that spans Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, Tennessee, and West Virginia – both adults (19.2% vs. 13%) and young adults (11.2% vs. 7.6%) have 50% higher smoking prevalence and smoke many more cigarettes per capita annually than people living in other states (on average, 53 vs. 29 packs). That means a smoker living in Tobacco Nation could smoke nearly 500 more cigarettes per year than the average smoker in the rest of the U.S.
In 12 states – a region we call “Tobacco Nation” that spans Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, Tennessee, and West Virginia – both adults and young adults have 50% higher smoking prevalence and smoke many more cigarettes per capita annually than people living in other states.
This persistently high prevalence of cigarette use – still the country’s leading cause of preventable death and disease – has serious consequences, especially at a time when life expectancy has declined for Americans due to a variety of factors including COVID-19 and opioid overdoses. Tobacco Nation residents live shorter lives and face a higher risk of dying than other Americans, with an average life expectancy of 76 years compared to 79 years in the rest of the country. Tobacco Nation’s greater rates of smoking-attributable death and disease compared to the rest of the U.S. likely contribute to this lower life expectancy.
Yet it is possible to create a future where these geographic disparities do not exist anymore. According to a separate analysis by Truth Initiative® and HealthPartners Institute, more tobacco policy spending paired with higher cigarette taxes targeted to areas with the highest smoking prevalence can reduce disparities in tobacco use that have existed for decades, bringing adult smoking in Tobacco Nation down to the national average and resulting in considerable health and economic benefits. Specifically, the analysis predicts that implementation of key tobacco policy changes could lead to roughly 100,000 fewer cancer cases, 730,000 fewer hospitalizations, and 170,000 fewer deaths attributed to smoking in the first two decades following policy change as well as saving over $24 billion in smoking-attributable medical costs and increasing productivity by over $100 billion.
Researchers and policymakers have created a road map to end unequal smoking prevalence across the country. Why, then, has it been such a challenge to implement these policies? Disparities in tobacco prevention and cessation measures in Tobacco Nation are not the fault of the region’s residents. Residents of Tobacco Nation have historically supported policies at levels equal to their counterparts in states outside Tobacco Nation. Instead, strong tobacco policies have not gained traction due to a combination of factors, including lack of political will, powerful tobacco industry interference in legislation, and prevention of local jurisdictions from adopting strong tobacco prevention and cessation measures. These obstacles have become evident in recent years as strong local laws restricting the sale of flavored tobacco products, including menthol cigarettes and youth-appealing flavored e-cigarettes, have continued to gain momentum across the country, but very few have been implemented in Tobacco Nation. For example, only three out of nearly 400 flavored tobacco policies in the U.S. have been enacted in Tobacco Nation.
The research points to a clear need for action: without interventions, adult smoking prevalence in Tobacco Nation states is forecasted to be over 40% higher on average over the next 20 years compared to other U.S. states. Steps taken at the federal level – including the Food and Drug Administration’s proposed rules to remove menthol cigarettes and flavored cigars from the market – will likely have large impacts in Tobacco Nation states, but need time to take effect. In the meantime, local and state level protections – including prioritizing tobacco program spending in existing budgets, higher tobacco excise taxes on tobacco products, stronger local tobacco policies supporting smoke-free environments, and restrictions on the sale of flavored tobacco products – are needed to address long-existing inequities in smoking rates and health outcomes in our country.
More tobacco policy spending paired with higher cigarette taxes targeted to areas with the highest smoking prevalence can reduce disparities in tobacco use that have existed for decades, bringing adult smoking in Tobacco Nation down to the national average and resulting in considerable health and economic benefits.
AN UPDATE ON TOBACCO NATION TODAY
Tobacco use has significantly declined in the United States, with high school student smoking prevalence dropping from 28% in 2000 to 2% in 2022. Much of this decline is attributed to tobacco policy efforts, including price increases, smoke-free air laws, and youth access restrictions, as well as mass media public education and prevention campaigns. However, reductions in tobacco use have not occurred equally across U.S. populations and there are substantial geographic and sociodemographic disparities in tobacco use and associated health outcomes. New issues with uneven implementation of local flavored tobacco policies threaten to exacerbate the situation further.
Smoking prevalence in Tobacco Nation remains higher than the rest of the nation
Tobacco use is disproportionately high in several U.S. states – particularly in the South and Midwest. In our 2017 report, “Tobacco Nation: The deadly state of smoking disparity in the U.S.,” we highlighted a group of 12 states in this region, all of which had higher smoking prevalence than the national average: Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, Tennessee and West Virginia. We called these states with very high smoking prevalence “Tobacco Nation.” These states not only have a high prevalence of tobacco use, they also tend to have worse indicators of health, socioeconomic status, and coverage by tobacco policies. Our 2019 follow-up report “Tobacco Nation: An ongoing crisis” found that most smoking, demographic, and health characteristics remained largely unchanged and looked beyond the most current annual estimates to examine trends in smoking over time. It identified the same 12 states as the first report, plus South Carolina, as states that had consistently ranked in the top 25% of U.S. adult smoking since 2011.
This year, we once again identified areas of the U.S. where smoking prevalence among adults was consistently high between 2011 and 2020. Today, Tobacco Nation is comprised of the same 12 states we identified in 2017— Alabama, Arkansas, Indiana, Kentucky, Louisiana, Michigan, Mississippi, Missouri, Ohio, Oklahoma, Tennessee, and West Virginia — with smoking prevalence within the top quarter of adult smoking prevalence in the country. We flagged three additional states to monitor – Alaska, South Dakota, and Wyoming – that may be on the verge of joining Tobacco Nation. While South Carolina, which was included in our last report, still has higher smoking prevalence than the national average, it did not consistently rate in the top 25% of smoking prevalence for states in the period we examined.
Although smoking prevalence has declined across the U.S. since our 2019 report, residents of all ages in Tobacco Nation are still more likely to smoke than residents living in the rest of the U.S. Smoking prevalence is about 50% higher in Tobacco Nation compared to the rest of the U.S. among both adults (19% vs. 13%) as well as young adults (11% vs. 8%). Youth in the region have a higher prevalence of cigarette smoking compared to the rest of the U.S. as well (6% vs. 4% in 2019). Not only is there a higher smoking prevalence among Tobacco Nation’s residents of all ages, they also smoke nearly twice as many cigarettes per capita annually (53 packs vs. 29 packs) than those in the rest of the U.S., amounting to nearly 500 more cigarettes a year.
With more than 67 million residents, these states include roughly 21% of the U.S. population but represent more than 28% of all adult current smokers in the country. When compared to the rest of the U.S., residents of Tobacco Nation states are less educated, not as financially well-off, and less likely to be employed, especially in white-collar jobs — trends we noted in our first Tobacco Nation report that remain true today.
What we know about e-cigarette use in Tobacco Nation
Since our first report in 2017, e-cigarettes have grown in popularity among youth and today are used by 14.1% of U.S. high school students. E-cigarettes, which come in a variety of youth-appealing flavors, are widely popular across sociodemographic groups, with alarming prevalence of youth use across all parts of the country. However, geographic patterns of adult e-cigarette use are more clear: according to the CDC, nine Tobacco Nation states report adult e-cigarette use prevalence that falls within the top 25% of all U.S. states.
It is not yet clear how youth vaping will contribute to tobacco-related disparities we see in Tobacco Nation states. We do know that the impact of new nicotine products is especially concerning in areas where tobacco use is normalized with high prevalence of adult e-cigarette and cigarette use, and where local or state policy protections are scarce. For example, while hundreds of communities recently enacted flavored tobacco product sales restrictions which include flavored e-cigarettes, only three of these policies have been passed in Tobacco Nation. E-cigarette use in Tobacco Nation presents cause for concern and calls for additional monitoring in the future, especially given strong evidence that young people who use e-cigarettes have much higher odds of later becoming smokers compared to those who have never vaped.
Higher smoking prevalence translates to poorer health
We know that smoking is much more prevalent in Tobacco Nation than other states, so what does that mean for the health of its residents? The numbers show us that where tobacco use is high, tobacco-related health conditions and diseases are high, too. Not only does smoking raise the risk of lung and bronchus cancer, it also raises the risk of developing heart disease. Since our last report, we saw nationwide declines in life expectancy and increases in mortality from conditions like heart disease and cancer. However, given the number and frequency of cigarettes smoked in Tobacco Nation, it is both dismaying and unsurprising Tobacco Nation residents are more likely to die from cancer, heart disease, and chronic lower respiratory disease than those living in the rest of the U.S.
Where tobacco use is high, tobacco-related health conditions and diseases are high, too. Not only does smoking raise the risk of lung and bronchus cancer, it also raises the risk of developing heart disease.
More smokers in Tobacco Nation also suffer from other health conditions that accompany tobacco use compared to the general adult smoking population. For example, 26% of smokers in Tobacco Nation report excessive drinking compared to 17% of its total adult population. Smokers in Tobacco Nation also report much higher rates of frequent physical distress, diabetes, poor physical health days, physical inactivity, and chronic obstructive pulmonary disease compared to the total adult population.
Life expectancy across geographic areas is highly correlated with preventable health behaviors such as smoking. In cities with highly educated populations, high incomes and high levels of government spending, individuals with low incomes live longer, report greater physical and mental health, and have healthier behaviors. In places where government support is relatively high and public policies encourage better health for all, its poorest residents fare better than similar residents living in other parts of the country. Conversely, in areas with a high prevalence of smoking and low levels of government spending, low-income individuals have the shortest life expectancy. In these areas, the deck is stacked against them. This adds up to a stark reality for residents of Tobacco Nation who are in areas of greatest smoking prevalence and with typically lower levels of government spending. This reality has become even more apparent throughout the COVID-19 pandemic. Tobacco Nation residents live shorter lives than other Americans, with an average life expectancy of 76 years compared to 79 years in the rest of the country.
Tobacco Nation fares worse in mental health declines
In addition to life expectancy, mental health has declined across the country (in part due to the COVID-19 pandemic) but indicators remain worse in Tobacco Nation than other U.S. states. Adults in Tobacco Nation more often report poor physical and mental health days and report more frequent mental and physical distress compared to the rest of the U.S. Tobacco Nation’s smokers are also more likely to report frequent mental distress (26.9%) than the average Tobacco Nation resident (16.1%). The story is similar for poor mental health days.
This disparity is concerning given the relationship between mental health and nicotine. Individuals with mental health conditions are more likely to report smoking and smoking in greater amounts. In turn, evidence suggests that nicotine can intensify symptoms of anxiety and depression.
The connection between COVID-19, mental health, and smoking
Since our last report, COVID-19 has affected the health of individuals across the globe. From 2019 to 2021, life expectancy in the United States declined by 2.7 years – the largest two-year drop since the 1920s – with much of this decline attributed to COVID-19 deaths. In addition, mental health has also declined in the U.S. which seems to have been heightened by COVID-19. This has been particularly true among youth, with 37% of U.S. high school students reporting poor mental health most of the time or always during the COVID-19 pandemic. Against this backdrop of worsening health indicators, disparities persist between Tobacco Nation and other states.
Because the virus that causes COVID-19 attacks the lungs, the pandemic intensified concerns about the impact of smoking on health. Similarly, declines in mental health during the COVID-19 pandemic raise concerns about the relationship between mental health, tobacco use, and difficulties with quitting tobacco. This is especially true in Tobacco Nation, which has some of the highest smoking prevalence in the country. According to CDC data, nine of the 12 Tobacco Nation states fall within the top 25% of state-level COVID-19 death rates. Individuals in Tobacco Nation also report poorer mental health, on average, than residents of other states.
Lyme disease is caused by the bacterium Borrelia burgdorferi and is transmitted to humans through the bite of infected black-legged or deer ticks. It’s typically treated with antibiotics as the standard course of therapy.
Despite the growing threat, “less than half of people even know they had a tick bite,” says Dr. Schweig. Symptoms to look out for include a rash, headache and stiff neck. Up to 20% of patients develop chronic Lyme, with symptoms like fatigue and brain fog. “Once it’s longer-term, it’s very difficult to cure,” says Dr. Schweig.
If you suspect Lyme, find a doctor versed in treating it. Experts advise getting the ELISA antibody test and the Western Blot. But the tests aren’t perfect, says Dr. Schweig. If you have a rash and think you were bitten by a tick, he advises taking antibiotics for two to three weeks, even if you test negative. “You want to be very aggressive to eradicate that bug.”
How to treat Lyme disease with biomagnetic therapy
They’ve been used for decades to help ease pain, but experts who treat chronic Lyme disease use a different type of magnetic energy to help their patients. Biomagnetic therapy uses two magnets with opposite magnetic fields placed on body parts where some type of imbalance has been found, says Heather Tallman Ruhm, MD, of the New Hampshire Health & Wellness Center in Nashua, New Hampshire. The technique hasn’t been well-studied, but she says, “The magnets seem to balance and restore optimal pH levels, which supports the body’s innate capacity to heal from pathogens, emotional imbalances and other conditions.”
Lyme disease success story: How Rebecca found relief
For eight years, Rebecca Powers Tibball, 49, fought fatigue, fog and pain caused by Lyme disease. Then she found an unusual remedy that helped her heal.
“Another day, another thing stripped away from me,” Powers Tibball recalls of the day she quit the job she’d loved for 14 years as an elementary school teacher due to the debilitating effects of chronic Lyme disease.
“Soon after spinal surgery in January of 2015, I developed constant dizziness and migraines, joint pain, neuropathy, nausea and light sensitivity. I also started losing weight and feeling depressed and tired all the time.
Rebecca’s Lyme disease diagnosis
“I saw 14 doctors in 10 months, including a neurology specialist at Yale-New Haven, an ear, nose and throat doctor and a thyroid doctor. I developed anxiety because I felt like I was losing my mind. No one could tell me anything. They were very nice, but very dismissive. No one had any idea what was causing this.
“At one visit, a chiropractor said, ‘Everything you’re saying sounds like Lyme disease.’
I was thrilled to hear this: Could I finally have an answer? And when I looked it up to investigate further, the list of symptoms was everything I had.
Searching for answers
“It took me four months to get an appointment with a physician specializing in the disease. He did extensive blood work that was analyzed at Stony Brook University’s Lyme Disease Laboratory. The results showed Lyme disease and other tick-borne illnesses, including babesiosis and Rocky Mountain spotted fever. I felt so validated that I wasn’t crazy.
“The doctor started me on antibiotics, but they made me so sick. I had dizziness, I couldn’t eat, the slightest sound overwhelmed me and my eyes and face swelled. I became bedridden. I felt worse than ever. I’d been on antibiotics for two months when my husband said, ‘Enough, no more antibiotics.’
Natural Remedies can help
“Lyme disease is an epidemic that is well recognized on the East Coast and less recognized across the rest of the country,” says Sunjya Schweig, MD, a Lyme expert in California and an advisory board member of the Bay Area Lyme Foundation. Indeed, infections have been found in every state, with cases doubling from 1990 to 2020.
So how to treat Lyme disease?
Antibiotics are the standard course of therapy, but for some, they don’t provide relief. That’s why many with chronic Lyme disease are turning to bio magnetic therapy. It worked for Rebecca Powers Tibball after eight years of suffering. Read on to learn more about the therapy and how it helped Rebecca heal.
The common name for skullcap used in America was “mad dog” during the 19th century because of its ability to heal animals and humans from rabies. Other popular names include skullcap, hoodwort, quaker bonnet, helmet flower, blue pimpernel, hooded willow herb and mad weed.
In addition to its reputation as an effective remedy against rabies, skullcap was used by Native Americans to promote menstruation. A root extraction was often taken after childbirth to help heal the reproductive system.
The Iroquois used it to keep the throat clear and healthy, and it was used to induce visions as a ceremonial plant to be smoked by some Native Americans.
Chinese physicians are known to have used the root, called huang qin, for antibacterial purposes, as a diuretic, an antispasmodic and to help with bile flow.
And in Nepal, the plant is used as a folk remedy for the common cold, cuts and insect stings. Additionally, some homeopaths have indicated it as a treatment for chronic fatigue syndrome and even epilepsy.
Benefits
1. May Help Fight Cancer Cells
Research shows that Chinese skullcap extract is toxic to cancer cells, such as brain tumor cells, prostate cancer cells, and head and neck squamous cell carcinoma cell lines. Studies indicate that aqueous extracts suppressed the growth of lymphoma and myeloma cells.
It’s believed that certain flavones, which are antioxidants within the plant, are responsible for these anticancer effects, ultimately inhibiting the growth. This may happen due to the free radical scavenging characteristics it contains, which prevents viral infections.
One of these flavones is known as baicalein. In a study published in the Beijing Science Bulletin, it appeared as though the baicalein did not cause any mutations, which is a serious problem of many conventional anticancer drugs available today.
Another study published in the International Journal of Molecular Medicine investigated the effects of the extract from skullcap on fibrosarcoma (a highly metastatic cancer of the connective tissue) and showed possible anticancer characteristics.
The rate at which cancer cells grew was significantly suppressed by treatment through apoptosis, and the volume and weight of tumors were greatly reduced as well. It appears as though the plant helped prevent further inhibition and migration of cancer cells, indicating its potential as a natural cancer treatment.
2. Calms Anxiety as a Nerve Tonic
For more than two centuries, the American skullcap has been used by both Americans and Europeans as a nerve tonic to help treat anxiety. Research has shown that the plant contains “anxiolytic activity” in animals and humans.
Oxidative stress affects some brain-related diseases, such as anxiety, Alzheimer’s disease, depression and Parkinson’s disease, yet research indicates that bioactive compounds found in medicinal plants, such as skullcap, may neutralize and even eliminate toxic free radicals.
When this occurs, oxidative stress is greatly reduced. Skullcap for anxiety may work because of its ability to provide significant antioxidant effects, which could make it a great option for reducing anxiety.
“Then I tried natural strategies, from the homeopathic remedies a naturopath recommended to bee venom and Rife therapy or healing with sound frequency.
It sounds kooky, but I slowly started to feel a little better.
I was able to return to teaching in September of 2018.
“One day, a friend told me about a friend of hers with Lyme disease who went to a magnetic therapy practitioner in New Hampshire. She said, ‘He’s all better. He’s exercising, he’s working.’ I was like, ‘Oh my God, I need to go.’ I thought it sounded wacky, but when you’re as sick as I was, you’ll do anything.
“There was a two-year wait for an appointment, but in a stroke of luck, the practitioner, Janelle Salzman, got me in within four months, and in June of 2022 I had my first visit.
“Janelle uses the “Lyme Magnetic Protocol Therapy, which means putting magnets on different parts of the body. It’s believed the magnets rebalance the body’s pH levels, which helps the immune system fight the disease.
If someone is considering this therapy, it’s recommended to consult with a healthcare provider who is knowledgeable about Lyme disease and its treatments. Additionally, it’s crucial to continue with any prescribed treatments and follow the advice of a medical professional.
Lyme disease relief at last
“I walked into her office with my mom and I broke down crying. Janelle was welcoming and warm and said, ‘You’re going to get better.’ I immediately stopped all of the other treatments and went to Janelle twice a month. The $200 treatments were an eligible expense for my insurance’s flexible spending account, and they were worth every penny.
“I would go in with brain fog and over the next week or two, notice that my thinking was clear. My appetite came back, my energy was restored. When you live with vague symptoms like I had, you feel crazy. Many practitioners make you feel like you’re nuts — that it’s all in your head.
“After six months, I was healed.
Today, my blood work shows zero tick-borne diseases. I don’t want anyone to go through what I went through, so I became certified to perform this therapy on others. Now I see patients with Lyme disease and other ailments at my healing center in Berlin, Connecticut. I love helping others. I feel so blessed.”
Marshallese youth in Celina are attending language classes, like this one in November, to preserve their Pacific Island culture. Michael Capelle has spent much of his life listening to the stories of older relatives reminiscing about life in the Marshall Islands. Capelle has never visited, but his parents have passed down its traditions and history.
The Marshall Islands, officially the Republic of the Marshall Islands, is an island country west of the International Date Line and north of the equator in the Micronesia region in the Northwestern Pacific Ocean. The territory consists of 29 coral atolls and five islands, divided across two island chains: Ratak in the east and Ralik in the west. 97.87% of its territory is water, the largest proportion of water to land of any sovereign state.
The country shares maritime boundaries with Wake Island to the north,
Kiribati to the southeast, Nauru to the south, and the Federated States of Micronesia to the west. The capital and largest city is Majuro, home to approximately half of the country’s population. “We sail around the seas, and we don’t need navigational tools. That’s what sets us apart,” he said. “We’re the people of the sea.”
Landlocked Ohio looks a lot different. Still, a small community of islanders made the long trek from the Marshall Islands – a country of 42,000 people that sits a couple thousand miles northeast of Papua New Guinea – to Celina, a small city in western Ohio, where Capelle lives. Despite the massive distance, Capelle is working to ensure the islands’ culture is passed onto the next generation growing up in Ohio.
Passing on the language
Around 30,000 people have emigrated from the Marshall Islands to the U.S. There’s no official count on their numbers in Celina, but city officials estimate around 1,500 Marshallese people live in the community. Capelle thinks it’s double that. The younger generation here is growing, he said, but their knowledge of Marshallese culture is fading.
“We can’t get to the point where our kids, all of them, don’t know how to speak Marshallese, they don’t know our stories, and they don’t know our values,” Capelle said. Michael Cappelle hands a green composition notebook to a teenager, while other students write at a table. He’s helping the student translate a sentence into Marshallese at a language class in November.
Michael Cappelle helps a student translate a sentence into Marshallese
at a language class in November.
So, in October, Capelle founded the Ohio Marshallese Youth Center.
On a Saturday night in November, nine teenagers are huddled around a table, scribbling notes and sipping Kool-Aid. Their attention is turned to a Zoom screen where Romaldo Kon Kabua, an instructor from Pacific Island Linguistic Services, is teaching them ways to greet each other in Marshallese: How to say hello, how are you, where they’re from.
But he’s not just offering translations. He’s teaching them about the islands’ matriarchal clans, the values of their ancestors, the traditions behind the text.
“Our greeting was very powerful, intentional, filled with love, filled with beauty,” Kon Kabua said, explaining the meaning behind “lakwe,” a greeting that literally translates to “you are a rainbow.”
Protecting a culture
Preserving this culture is difficult but important, said Capelle, especially because many Marshallese people didn’t choose to come to the U.S. Decades ago, they were displaced.
In the 1940s and 50s, the U.S. used part of the islands to test nuclear weapons. In Operation Crossroads, the United States relocated the tiny population of islanders from Bikini Atoll, a remote corner of the country, and detonated more than 200 million tons of TNT.
A dense cloud of smoke erupts from an atomic detonation at Bikini Atoll within the Marshall Islands. United States Department of Defense.
The detonation of atomic weapons in the Marshall Islands in “Operation Crossroads”
has left a devastating legacy on the small nation in the Pacific.
Those detonations have done lasting harm to the islands. Atomic radiation has damaged its population’s health, the islands’ environment and the Marshallese people as a whole. It contributed to emigration from their native land and subsequent erosion of the language skills that Capelle is seeking to preserve. The class is just one way that Capelle hopes to help reverse the gradual erasure of their culture.
“We’re thinking about getting to the high schools, getting to the government levels and showcasing our culture because we’ve had that question like, ‘Can you guys come and show us who you guys are?’” Capelle said.
A place for pride
Many of the students in the class said they speak Marshallese at home with their families, but beyond that it’s hard to find spaces to connect with their culture. That’s true for Emiko Ysawa, a 17-year-old who moved to Ohio seven years ago.
She joined the new language class so she could understand her “manit.” That’s the Marshallese word for “culture,” but it means more than that. One Marshallese essayist describes it as “the core of our being, the spirit in our walk.”
“As kids in this generation, we don’t really follow that expectation, and we just ignore it,” Ysawa said. “So for us to spread it out, we need to learn more about it.” Two teenagers write down notes in a composition book at a Marshallese language class in Celina.
Teenagers in Celina use this class as a way to not only practice their language skills,
but learn about the cultural stories and values of their homeland.
Her classmate Kayla Edejer agreed. The 14-year-old said leaving her home country was difficult. She’s grateful for the opportunity to keep in touch with its culture and ensure she has the language skills to talk with her family that remains there.
“I love how they reassure us, and they make sure that we feel comfortable in our own space and in this room,” Edejer said.
Capelle founded the Ohio Marshallese Youth organization so his young students can learn to find joy from their heritage, he said. He wants to continue to build places where pride in their home country is not just possible, but applauded.
“The Marshall Islands could sink, but I feel like it would always be with me,” Capelle said. “The Marshall Islands is not a land, it’s almost just a people.”
By Breaking News Staff January 05, 2018, at 2:07 pm EST
Far from home: Marshall Islands community in Ohio.
The Marshall Islands, a chain of atolls and volcanic rocks in the Pacific Ocean, are far from the city of Celina, Ohio. Forced to migrate, more than a thousand Marshallese now make their home in the landlocked state. The Ohio Newsroom’s Kendall Crawford reports on how the community is keeping their heritage alive.
The Marshall Islands community in Ohio, particularly in the city of Celina, has been making significant efforts to preserve their culture and language. Despite being thousands of miles away from their Pacific homeland, the Marshallese in Celina are attending language classes to keep their traditions alive1.
Michael Capelle, a local resident, has been instrumental in these efforts. He founded the Ohio Marshallese Youth Center to teach the younger generation about their heritage, including the Marshallese language and the values of their ancestors1. This initiative is crucial as many Marshallese were displaced to the U.S. due to nuclear testing on their islands by the U.S. in the 1940s and 50s1.
Are there any cultural events or festivals organized by the Marshall Islands community in Celina?
Yes, the Marshall Islands community in Celina, Ohio, organizes cultural events and activities to share their heritage. One such initiative is the Marshallese Culture Club, which meets weekly1. The club focuses on teaching the language, customs, and traditions of the Marshallese people. This includes learning about the islands’ matriarchal clans, the values of their ancestors, and the traditions behind their greetings and interactions2.
Additionally, the Ohio Marshallese Youth Center was founded to help pass on the language and culture to the younger generation growing up in Ohio2. They organize language classes and cultural lessons to ensure that the children do not lose touch with their roots2.
These efforts are part of a broader movement to protect and preserve Marshallese culture far from its Pacific Island origins, especially considering the historical displacement of many Marshallese due to nuclear testing on their islands2. The community’s dedication to maintaining their cultural identity is evident in these regular gatherings and educational programs.
The Marshall Islands, located in the central Pacific Ocean, consist of more than 1,200 islands and islets in two parallel chains of coral atolls: the Ratak (Sunrise) to the east and the Ralik (Sunset) to the west. These low-lying coral atolls and islands are composed of coral caps set on the rims of submerged volcanoes that rise from the ocean floor1. Here are some interesting facts about the Marshall Islands and their volcanic features:
Overall, 48 volcanoes were in continuing eruption status as of 19 April 2024. An eruption marked as “continuing” does not always mean persistent daily activity, but indicates at least intermittent eruptive events without a break of 3 months or more. There are typically 40-50 continuing eruptions, and out of those generally around 20 will be actively erupting on any particular day (though we do not keep detailed statistics on daily activity). Additional annual eruption data is available for recent years.
The Smithsonian / USGS Weekly Volcanic Activity Report (WVAR) for the week ending on 21 May 2024 includes the 27 volcanoes shown below marked “Yes” in the WVAR column (rollover for report). The most recently started eruption is at the top, continuing as of the Last Known Activity date. An eruption listed here might have
None of the 29 low-lying coral atolls and the five coral islands in the Marshall group rise to more than 20 feet (six meters) above high tide.
The islands are coral caps formed on the rims of submerged volcanoes that rise from the ocean floor.
The largest atoll in the group is Kwajalein, which surrounds a 655-square-mile lagoon and has a land area of only six square miles.
The Marshall Islands’ nearest neighbors include Wake Island (north), Kiribati and Nauru (south), and the Federated States of Micronesia (west).
The climate is tropical, with a mean annual temperature of 82°F (28°C) and varying annual precipitation1.
Seamounts and Volcanoes:
The Marshall Islands are the site of several seamounts (underwater volcanic mountains).
These seamounts form part of a larger province extending from the South Pacific to the Mariana Trench, characterized by unusually shallow ocean ground.
Some seamounts in the Marshall Islands do not follow simple hotspot-like age progressions; their volcanic activity episodes can be complex.
The largest seamount is Kwajalein, which has a land area of only six square miles but surrounds a 655-square-mile lagoon.
Other notable seamounts include Aean̄-Kaņ, Neen-Koiaak, Wōd-Eņ Rok, and Wōd-Eņ Iōn̄2.
Specific Seamounts:
Aean̄-Kaņ: Located at 14°52.98′N, 160°27.38′E, this seamount has a depth of 850 meters (2,790 feet) and dates back to the Mid-Cretaceous. It is the largest in terms of volume, with 10,389 cubic kilometers.
Neen-Koiaak: Situated at 14°22.62′N, 161°01.16′E, this seamount reaches a depth of 1,025 meters (3,363 feet) and is approximately 102 million years old. It contains Hawaiite rock. – Search (bing.com)
Wōd-Eņ Rok: Found at 15°13.20′N, 163°00.00′E, this seamount is about 76 million years old and is a candidate member of the Ralik hotspot trail.
Wōd-Eņ Iōn̄: Located at 16°06.00′N, 163°02.40′E, this seamount is approximately 86 million years old and also a candidate member of the Ralik hotspot trail2.
In summary, the Marshall Islands are not only a tropical paradise but also home to fascinating underwater volcanic features that shape their unique landscape.
Traditional Marshallese cuisine is a blend of indigenous fare and influences from other cultures. Here are some of the staple foods and dishes:
Breadfruit: Often used as a staple food, it can be roasted or mashed1.
Coconut: Utilized in various forms, including the meat and milk1.
Bananas and Papaya: Commonly consumed fruits1.
Seafood: Including fish, coconut crab, and clams, given the islands’ location in the Pacific1.
Pandanus: A type of fruit used in many dishes1.
Bwiro: A traditional dish consisting of fermented breadfruit paste wrapped in banana leaves and cooked in an underground oven1.
Additionally, some of the national dishes and popular foods include:
Barramundi Cod: Seasoned and wrapped in banana leaves, then baked2.
Chukuchuk: Rice balls rolled in freshly grated coconut2.
Sweet Potatoes & Fried Bananas: Boiled sweet potatoes and bananas fried in coconut oil2.
Rice-banke: A simple dish of diced pumpkins and rice, sometimes with coconut milk2.
Marshall Islands Macadamia Nut Pie: A dessert pie made with macadamia nuts, corn syrup, sugar, and vanilla extract, topped with coconut whipped cream2.
These foods not only provide sustenance but also hold cultural significance, often playing a role in celebrations and special events1.
Tell me more about the traditional cooking methods in Marshall Islands.
Traditional cooking methods in the Marshall Islands are deeply rooted in the islands’
culture and natural resources. Here are some key techniques:
Earth Ovens (Ums): A common method is using earth ovens, known locally as “ums.” Food is wrapped in leaves and slow-cooked over heated rocks buried in the ground. This technique allows for a slow, even cooking process that infuses the food with a smoky flavor1.
Open Flame Cooking: Another prevalent method is cooking over an open flame. It’s a straightforward approach that imparts a distinct smoky taste to the food1.
Sun-Drying: For preserving fish, sun-drying is a traditional technique. The fish is cleaned, salted, and then dried under the tropical sun, which creates a storability and intensifies the flavor1.
Grilling on a Men: The traditional grill, called a “men,” is made from coconut leaves. It’s used to cook fish, meat, and vegetables over hot coals, giving the food a unique smoky essence2.
These cooking methods not only prepare the food but also preserve the cultural heritage of the Marshallese people, showcasing their ingenuity and connection to the environment.
Clifford Joseph displays a Haitian flag on his desk in his North West Street office in Lima. Joseph has been a point of contact for Haitians wanting to make a new life in the Lima area.
LIMA — Walk along the produce section of a small grocery store on the corner of West Spring Street and Jameson Avenue and you will find some familiar items, like yams or even plantains, but you will also find such items as malanga, a root vegetable, or a bag of lalo, or dried jute leaves. Look a little farther and you will come across items like cassava bread or jasmine rice, along with spices like cinnamon sticks and star anise.
If you have any questions, however, knowing some Creole French would be helpful.
This store is helping what is becoming an increasingly large Haitian population in the Lima area find some tastes of home as they work to make a new life for themselves in west central Ohio. As conditions deteriorate and violence rises in the small Caribbean nation, more Haitians are seeking refuge in the United States, hoping to find an escape from the violence and poverty that has stricken their home.
“From what I’ve heard from other Haitians, usually Haitians will be in the northeast, especially Brooklyn, or in Florida,” Lima psychiatrist Dr. Eddy Bruno said. “In fact, at some point, either Brooklyn or Miami have more Haitians than the second [largest] city in Haiti.”
What is bringing Haitians to Lima?
A native of Haiti, Bruno has lived and worked in Lima for nearly 20 years. While he will say he is not the first Haitian to live in Lima, he was one of only a few in this area for some time, he said. However, he is now seeing a shift as more Haitians find themselves in Lima and the surrounding area, with some having been first in the Springfield area and then migrating to Lima.
“I’m not sure how it happened, but it seems like that even when they’re trying to make it to the States, they’re hearing that the Midwest has more jobs and more opportunity,” he said. Bruno also cited the area’s lower cost of living as a draw for those in the Haitian community.
For John Noel, the owner of the Spring Street grocery store, that is what brought him to the area, having lived first in Columbus before moving to Lima two years ago. “Haitians are everywhere in the United States,” he said. “They need the jobs, so they come and get the jobs. They like to work.”
What challenges do they face?
That goal of employment is not always an easy one for Haitians coming to the community with few resources and obstacles like language barriers to overcome. Born in Haiti but now working in Lima, Clifford Joseph operates an office to help Haitian arrivals work through obtaining needed documentation and point them toward resources linking them with food, housing and education, and this has proved difficult.
“They don’t have all their papers most of the time,” he said. “Sometimes they don’t even speak the language. That’s another problem. Most of the time, when they move here, they rent a room from someone but the lease is not in their name, so it’s not easy for them to register their kid for school because as soon as they go to the school, they want proof of living and stuff like that. In Florida or New York or Georgia, because there are already a lot of Haitians already established in the community, they know them, so it’s easier for them to find services.”
That difficulty has also been exacerbated by the large influx of Haitians, with Joseph estimating that about 5,000 Haitians have moved into the area over the last couple of years. “I know it’s not easy for a small city like Lima,” he said. “They didn’t build the city to receive that many people. Getting 5,000 people at once, it’s not easy.”
How is the community responding?
Some in Lima have been working to address that need, with representatives from Mercy Health-St. Rita’s Medical Center starting a dialogue over the past year with Activate Allen County and the Lima-Allen County Chamber of Commerce, as well as representation from such areas as city and county government, public health and education, to address how to best help these new arrivals.
“It started as a conversation sometime in the fall,” Mercy Health-St. Rita’s Director of Government and Community Relations Beth Keehn said. “In the last few months, it became more active just because I think all the groups are starting to feel that flux of refugees more rapidly than we had previously.”
According to Keehn, this conversation has been leading to the beginnings of a new initiative to address these issues. To this point, the work has consisted mainly of listening, whether it was to a refugee office in Columbus, to community leaders in Springfield or to the new arrivals themselves.
“What we believe some of the challenges they are facing are questions around how to navigate healthcare, transportation options, education, and that includes traditional education as well as a big desire to get into English language classes,” Keehn said. “Employment options are a question, and then certainly housing. We’re at the very early stages of this structure.”
Bruno and Joseph echoed some of those concerns, relating stories of Haitians facing exorbitant charges to get rides to jobs or paying as much as $600 every week for housing. “One thing we are hoping and praying is that these people won’t be taken advantage of, but this is something we are seeing a lot,” Bruno said.
Joseph emphasized that the people coming here are often not uneducated but often include lawyers, engineers, nurses or other professionals, all of whom had to leave to avoid the escalating violence in their homeland. “They come here just looking for a better opportunity,” he said. “They are not coming to do anything wrong.
All they want is a better living. They are hard-working. They are not looking for handouts.
There are also roughly 27,000 Marshallese citizens residing in the United States,[4] nearly all of whom speak Marshallese, as well as residents in other countries such as Nauru and Kiribati.
There are two major dialects, the western Rālik and the eastern Ratak.
The Haitian people primarily speak Haitian Creole and French1. Haitian Creole is the most widely spoken language, with more than 95% of the population fluent in it. It’s a unique blend of French, Taino, and some West African languages, reflecting the country’s diverse history and cultural influences2.
French, while being an official language and used in formal settings like education and media, is spoken fluently by only about 5% of the population, typically the elite and those in urban centers2. Other languages such as Spanish and English are also present in Haiti, especially near the border with the Dominican Republic and within the business community2.
How similar is Haitian Creole to French?
Haitian Creole and French share a historical connection, which is reflected in several similarities, but they are distinct languages with their own unique characteristics. Here’s a brief overview of their similarities:
Vocabulary: A significant portion of Haitian Creole’s vocabulary comes from French, although the pronunciation and sometimes the meaning of these words have evolved1.
Alphabet: Both languages use the Latin alphabet, making it easier for those literate in one to read and write in the other1.
Numerals: The numerical system in Haitian Creole is based on French numerals, so numbers are expressed similarly in both languages1.
Common Phrases: Some common French phrases and greetings are incorporated into Haitian Creole, often in a slightly modified form1.
Loanwords: For modern concepts, especially technical or scientific terms, both languages often borrow words from each other1.
Cognates: There are cognates—words that are similar in both languages and share a common origin—although their pronunciation and meaning may have diverged over time1.
Despite these similarities, Haitian Creole has its own grammar, syntax, and phonetics, which are quite different from French. This means that while someone who speaks French might recognize some words and phrases in Haitian Creole, they would likely find it challenging to understand or communicate effectively without learning the specific nuances of Haitian Creole2.
We keep trying to make sense of death because we’re afraid of it.
After all, how can we not be when all we have ever known is life?
It’s always scary to step into change, and the more unknown that change is, the more daunting and unpredictable it feels.
Thankfully as time has gone on and science has advanced, we have been able to make death less of a mysterious thing. We now have a better understanding of some of the eerie but fascinating things that happen in our final moments. Here are the 8 most notable things based on the experiences of people who died and then came back.
Almost everyone that had a near-death experience—meaning that their heart stopped beating and flatlined, only to be resuscitated once again,—reported an ability to step outside of their body.
They explained that not only were they able to see themselves as they were floating in space, but they were also able to give accurate details of who was around, what they were doing and saying, and what was happening during the moments they were technically clinically dead.
The expression “seeing the light at the end of the tunnel” didn’t come out of nowhere.
This raises questions as to whether our spirit is attached to our physical bodies or whether we float away from death when we die and go on to live in some sort of spirit world instead. Seeing a light upon death is a common report by those who were brought back away from it. Just like we have seen in the movies, it’s true that they describe feeling welcomed into a warm, bright, and beautiful light.
Everything Was Connected
The intensity of the brightness of that light differs from person to person. Some people have described that light as “God.” Some of those who had enough time to step into it also described finally getting the answers to all sorts of questions about the universe. They explained that everything was connected and that it all finally made sense. The light was so reassuring, that some didn’t want to be brought back to life.
You See Your Life Flash Before Your Eyes
Seeing your life flash before your eyes also is a true statement.
This phenomenon has been the subject of many scientific studies.
A recent study’s most notable discovery was that for about 30 seconds before and after a man’s heart stopped beating from cardiac arrest, activity increased in the parts of the brain associated with memory recall, meditation, and dreams. This information supports a theory known as”life recalls” which suggests that we relive our whole life in seconds, or a flash, just before we die.
Our eyes move rapidly, like REM sleep, while accessing memories. This shows that, as more and more studies are revealing, the brain remains active during and immediately after death. Perhaps one of the most heartwarming reports of what happens after death is that people report being able to see and interact with loved ones who have passed away, even if it’s for a short visit.
They can’t necessarily control who they will encounter
but oftentimes it’s a relative or dear friend who appeared to them.
Some have even been told to go back to life as it was not yet their time to join them in the afterlife. Perhaps our lost loved ones really are watching over us somewhere from beyond until we join them one day.
Almost every person who reported having a moment in which they were clinically dead, reported that they were able to float outside their physical body in spirit. This is something people have been trying to do while alive but sleeping, calling it astral projection.
Astral Projection
Astral projection is a practice of leaving the body safely. There are numerous guides that teach people how to leave their bodies on command. It starts out by practicing lucid dreaming, or the ability to control your dreams. While this may be experienced differently when sleeping versus when dead, it can simulate the experience to give you an idea of what to expect!
One of the fascinating discoveries is of people reporting being able to see and hear everything that happened around them while they were unconscious even though they weren’t able to respond.
Sixth Sense
One person, in particular, mentioned that they were able to see the green-haired paramedic that was sitting by them as they lay unresponsive. Days later, upon gaining back consciousness, she saw him again in real life. She approached him to ask. She said he seemed astonished because there was no way she should have been able to see him. Perhaps we tap into a sixth sense we’re not even aware of when we die.
There is no way to guarantee for sure what exactly will happen to each of us upon death. It’s possible that the experience will be relative to the person. Not all near-death experiences have been positive.
Some say that death was nothing but fading to black. In some cases, they said it felt like a deep sleep, without dreams.
This is the worst fear for some of us. It would mean that our whole lives end up being meaningless and truly end as our physical bodies decay. It’s hard to believe that our bodies simply rot and our souls along with them. But, this can also be motivation to live as full of a life as possible while we are still alive.
I have studied NDE’s and like flying paper airplanes no two experiences are the same.
This as-told-to essay is based on a conversation with Jeffrey Long. It has been edited for length and clarity.Thirty-seven years ago I was an oncologist resident, learning about how best to treat cancer using radiation. These were the pre-internet days, so I did my research in the library. One day I was flipping through a large volume of the Journal of American Medical Association when I came across an article describing near-death experiences.
It stopped me in my tracks. All my medical training told me you were either alive or dead. There was no in-between. But suddenly, I was reading from a cardiologist describing patients who had died, then come back to life, reporting very distinct, almost unbelievable experiences. From that moment, I was fascinated with near-death experiences or NDEs. I define a near-death experience as someone who is either comatose or clinically dead, without a heartbeat, having a lucid experience where they see, hear, feel emotions, and interact with other beings. Learning more about these experiences has fundamentally changed my view of the universe.
Near-death experiences have common threads
When I finished my residency, I started the Near-Death Experience Research Foundation. I started collecting stories from people who had NDEs and evaluating them with the mind of a scientist and doctor. I make opinions based on evidence and came into this as a skeptic. But in the face of overwhelming evidence, I’ve come to believe there’s certainly an afterlife.
I saw a consistent pattern of events, emerging in a predictable order. About 45% of people who have an NDE report an out-of-body experience. When this happens, their consciousness separates from their physical body, usually hovering above the body. The person can see and hear what’s happening around them, which usually includes frantic attempts to revive them. One woman even reported a doctor throwing a tool on the floor when he picked up the wrong one—something the doctor later confirmed. After the out-of-body experience, people say they’re transported into another realm.
Many passes through a tunnel and experience a bright light. Then they’re greeted by deceased loved ones, including pets, who are in the prime of their lives. Most people report an overwhelming sense of love and peace. They feel like this other realm is their real home. I haven’t found any scientific explanation for these experiences that may sound cliche: the bright light, the tunnel, the loved ones.
But over twenty-five years of studying NDEs. I’ve come to believe that these descriptions have become cultural tropes because they’re true. I even worked with a group of children under five who had NDEs. They reported the same experiences that adults did—and at that age, you’re unlikely to have heard about bright lights or tunnels after you die.
Other people report seemingly unbelievable events, which we can later confirm.
One woman lost consciousness while riding her horse on a trail. Her body stayed on the trail while her consciousness traveled with her horse as he galloped back to the barn. Later, she was able to describe exactly what happened at the barn because she had seen it despite her body not being there.
Others, who hadn’t spoken to her, confirmed her account. I’m a medical doctor. I’ve read brain research and considered every possible explanation for NDEs. The bottom line is that none of them hold water. There isn’t even a remotely plausible physical explanation for this phenomenon. I’ve also studied fear-death experiences, like near-miss car accidents.
I take a particular definition for NDEs. The person must be unconscious. But there’s another type of phenomenon that fascinates me too: what I call fear-death experiences. These are situations where you feel your life is in imminent danger. It might be a near-miss car accident or a sudden fall. These people generally don’t experience the tunnel and light, but they often report their life “flashing before their eyes.” While some people with NDEs report these life reviews, they’re more common with fear-death experiences. People even recall events from toddlerhood that they can’t consciously remember. But that we can later
confirm by talking with family members and others. Studying NDEs has made me a better cancer doctor. While I’m passionate about NDEs, my day job still revolves around helping patients fight cancer. I don’t tell my patients about my NDE research. And yet, my work with NDEs has made me a more compassionate and loving doctor. I’m able to help my patients face life-threatening diseases with increased courage and passion. My goal is to help them have more healthy days here on Earth. But I firmly believe that if and when they pass, they will be at peace.
A woman standing on top of a mountain to feel the human energy field
C.S. Lewis once said, “You don’t have a soul. You are a Soul. You have a body.”
Though it sounds rather religious or metaphysical, this statement is now backed up by science. At least partially.
Mind, Body Spirit Connection and Health – Think of a human being as a body-mind-spirit complex. These layers, known as the human energy field, are invisible and intangible, but they are essential for your well-being. If any of these are out of balance, they can manifest on a visceral level—as a physical ailment, emotional or mental distress, or a sense of disconnection with self or others.
But knowing how to balance them can level up your human experience.
We are much more than our physical body. The human energy system consists of much more than is perceived to our physical eyes. The human body consists of an electromagnetic energy field, which makes up for our subtle bodies, or Light Body, consisting of 7 Chakras and meridians through which energy flows. 47 Human Energy Field ideas | energy field, energy, energy healing (pinterest.com)
Also known as “aura” or “biofield,” the human energy field is an invisible energy surrounding the human body. It’s an integral part of many belief systems and alternative healing practices rooted in spiritual traditions. The human energy field has multiple layers—five of them—and each has its own function:
Physical: Directly connected to the physical body
Etheric: The blueprint for the physical body
Emotional: Contains emotions and feelings
Mental: Linked to thoughts, beliefs, and mental processes
Spiritual: What connects humans with the divine
The importance of the human energy field lies in the direct connection between energy and well-being. Because, at the end of the day, everything is energy. And by altering it, you can improve many different aspects of your life.
Humans have an energy field around them that can extend up to several feet from the physical body. If you search for human energy field images, most of them are pictured as egg-shaped cocoons around the body. The specific size varies, and it depends on factors such as health, age, emotions, and state of mind.
Generally speaking, the more positive your well-being is, the bigger your human energy is, and vice versa. Similarly, experienced energy workers and those engaging with spirituality usually have larger and more prominent auras.
What’s more, the size of each layer in the energy field also varies. The innermost layer, the one closest to the physical body, is also the smallest. And the outermost layer, which is the spiritual layer, is the largest.
The 5 Layers of the Human Energy Fields
Different belief systems and schools of energy healing may have slight variations in the number and attributes of the energy fields. That said, most systems have agreed upon these five layers of human energy fields.
1. The physical layer
This is your visceral body, composed of flesh, skin, bone structure, organs, and blood. It’s a physical representation of what you perceive as self. And for most people, it’s the only self-perception they have. Although you are quite aware of your physical body, your eating, drinking, breathing, and moving patterns leave much to be desired.
But if you don’t set them right, it will affect your mental, emotional, and even spiritual bodies. Jeffrey Allen, a world-renowned energy healer and author of Mindvalley’s Duality Quest, explains that when you go through painful experiences, you store energy from them in your body.
Whatever you store spreads out into the world through your process of self-expression. That’s why it’s so important to heal yourself, release negativity from your body and consciousness, and nurture it in ways that serve your highest good.
Achieving balance in your human body’s energy field comes with optimal health, energy, vitality, and resistance to illness.
Here are a few ways to keep your physical energy field balanced:
Healthy lifestyle. Eat a balanced diet, stay active, and get enough sleep.
Body awareness. Stay in tune with your physical sensations by practicing activities like yoga, Tai Chi, or body scans.
Energy healing. Massage therapy and acupuncture help release physical tension and promote energy balance.
Hydration. Don’t forget to stay hydrated during the day.
2. The etheric layer
The second layer surrounding your body is the etheric. It serves the role of a bridge between the physical and energetic realms of yourself. It’s also closely associated with the life force energy, often referred to as “prana” or “chi,” which is believed to flow through the energy meridians in the body.
This layer is considered a template or blueprint for the physical body. It contains the energetic patterns and information necessary for the physical body’s development, maintenance, and vitality. You can picture it as a web of energy that mirrors the body’s structure and functions.
How to keep a balanced etheric energy field
Your physical body needs to be in alignment with the energetic patterns and templates in the etheric layer. Thanks to this alignment, you can have a basis for the proper growth, development, and functioning of your physical systems.
For a balanced etheric energy field, you may want to practice these:
Grounding. Spend time in nature, practice earthing, or meditate to connect with the earth’s energy.
Energy cleansing. Use techniques like smudging, salt baths, or crystal cleansing to clear stagnant energy from your etheric field.
Pranayama. Explore yogic breathwork to enhance prana flow.
Mindful living. Practice mindfulness to stay present in the moment and maintain awareness of your energetic state.
3. The emotional layer
This is the layer where your emotions, feelings, and fears reside—it’s the most volatile layer of all. Although you are seemingly experiencing emotions inside, they are both inside and outside of you at the same time.
Jeffrey explains that people don’t allow themselves to feel their emotions out of fear of becoming them. But you aren’t your emotions.
He adds, “Emotions are the foundation of authenticity, and by allowing yourself to feel your emotions, you are helping yourself and others.”
How to keep a balanced emotional energy field
A balanced mental layer is characterized by clear and focused thinking, emotional stability, and reduced mental stress.
You can keep your emotional energy field in check with these practices:
Emotional awareness. Regularly check in with your emotions by acknowledging and processing them.
Self-expression. Express your feelings in creative ways, such as by keeping a journal or talking with a trusted friend, partner, or therapist.
Meditation. Incorporate this practice that focuses on emotional well-being, such as loving-kindness meditation.
Boundary setting. Set clear boundaries to protect your energy from emotional drains or conflicts.
4. The mental layer
Commonly referred to as your mindset, this layer is where all your ideas, thoughts, and belief systems are carefully stored, assimilated, and sorted out. It’s within your mental body that your truths and perceptions are formed, and often determines whether you remain stuck in life or propel you forward.
It’s crucial to understand that your mental body also serves as a filter between your mental and spiritual bodies. This intermediary role is often referred to as intuition, a vital link that connects you with higher consciousness.
So, it’s worth noting that your mental body doesn’t necessarily imply mental awareness. Instead, it’s primarily influenced by the programs, patterns, and belief systems you inherit, adopt in childhood, and develop during your life.
In other words, your mind can remain unaware, and an unaware mind can lead you into various predicaments because it gives you a feeling of being right all the time. What’s more, an unaware mind results in mental chatter, or noise, that keeps you stuck in negative scenarios, diminishing your mental clarity and focus.
The chakras and the limbic system are part of different conceptual frameworks and are not directly related. The limbic system is a set of brain structures that supports a variety of functions including emotion, behavior, motivation, long-term memory, and olfaction1. It is often referred to as the “emotional brain” and is highly involved in the body’s response to emotional stimuli.
On the other hand, chakras are part of an ancient Indian system of spiritual, physical, and emotional energy centers within the body2. They are not physical structures like the limbic system but are thought to be energetic focal points that influence various aspects of a person’s well-being.
While the limbic system is a well-defined group of structures within the brain studied in neuroscience, the concept of chakras comes from spiritual and holistic practices and is not recognized in the same way by modern science. However, some people believe that the state of one’s chakras can influence their emotional and physical health, which could be seen as a parallel to how the limbic system influences emotions and behaviors. But it’s important to note that this is a belief and not scientifically proven to be part of the limbic system or its functions.
‘PsyPost’ reports that scientists have uncovered how specific parts of the human brain require different amounts of energy than other parts. The work, which was published in ‘Science Advances,’ highlights how evolution of human cognition is linked to the development of energy-intensive brain networks.
Jeffrey explains that this chakra… Is about inspiration and spirit connection,
Connects you to the rest of the chakras, Is where you receive ideas, and store information about your past lives and connections.
“Your spirit connection is your sense of connection with others and the universe,” he adds.
However, when this energy point is blocked, people don’t believe that there’s something beyond them and that they are part of divinity. They often don’t trust their wisdom and higher guidance.
On the contrary, if you have a spiritual awareness, you live from that meta-understanding that you really are a spirit. You move along your life with a strong sense that everything is divinely orchestrated and works out for your highest good.
How to keep a balanced spiritual energy field
A balanced spiritual field is necessary for achieving inner peace, connection to the higher self, transcendence, and a clear sense of purpose.
For a balanced spiritual energy layer, exercise the below points regularly:
Spiritual practices. Engage in spiritual practices such as meditation, prayer, or contemplation to nurture your spiritual connection.
Introspection. Reflect on your spiritual beliefs, values, and purpose in life.
Connection. Create connections with like-minded individuals and join spiritual communities.
Compassion. Cultivate a sense of compassion, both for yourself and others, as part of your spiritual well-being.
Cancer is a complex disease with multiple causes, and while emotions and stress can impact overall health, they are not direct causes of cancer. The National Cancer Institute notes that while cancer can bring up a wide range of emotions and existing feelings may seem more intense, these emotions themselves do not cause cancer1. However, there is evidence suggesting that chronic stress and negative emotions can have an impact on the body’s immune system, which in turn could potentially influence the development of cancer23.
It’s important to understand that cancer is primarily caused by genetic mutations and can be influenced by various factors such as environmental exposures, lifestyle choices, and certain infections. Emotional health is crucial for coping with cancer, and addressing mental health concerns may lead to improved treatment outcomes and a better quality of life4. If you have concerns about cancer risks, it’s best to consult with a healthcare professional who can provide information based on medical evidence.
The Sedona vortex phenomenon, often associated with spiritual and mystical experiences, does have natural explanations that skeptics and scientists point to. The so-called vortexes are not scientifically recognized as distinct physical entities with measurable forces. Instead, they are areas within Sedona’s already stunning landscape that have been given special significance due to the feelings they evoke in visitors.
Here are some natural explanations for the sensations experienced at these sites:
Geological Beauty: The breathtaking red rock formations and scenic views in Sedona can naturally induce feelings of awe and tranquility, which may be mistaken for a spiritual or energetic experience1.
Psychological Effects: The power of suggestion and the human tendency to feel uplifted in beautiful natural settings can contribute to the belief in and sensation of vortex energy1.
Physical Activity: Hiking and being outdoors have well-documented mood-boosting and health benefits, which can enhance one’s sense of well-being when visiting these areas1.
Cultural Influence: The history of Native American reverence for these lands adds a layer of spiritual significance that can influence visitors’ perceptions2.
While the idea of vortexes as sources of unique energy is a popular aspect of Sedona’s allure, it’s important to note that there is no hard scientific evidence to support the existence of such forces. The feelings experienced by visitors are likely a combination of the natural beauty, cultural stories, and personal beliefs that converge in this unique location12.
The Sedona Vortexes are indeed a fascinating phenomenon. They are thought to be swirling centers of energy that are conducive to healing, meditation, and self-exploration1. Many visitors report feeling inspired, recharged, or uplifted after visiting a vortex in Sedona. The four best-known vortex sites are at Airport Mesa, Cathedral Rock, Bell Rock, and Boynton Canyon1. Each site is believed to radiate its own particular energy, with some producing energy flowing upward and others spiraling downward into the earth1.
Whether you’re on a journey of self-discovery or just looking to experience the natural beauty and serenity of Sedona, the vortexes offer a unique and potentially transformative experience. Remember to visit with an open mind and respect the practices and rituals of others you may encounter at these sites1.
Feeling anger over seemingly small issues can be a complex emotional response influenced by various factors. It’s often not just about the immediate situation but can be a result of underlying stress, anxiety, or other emotional challenges1. When people are under a lot of stress, they may have a heightened “fight or flight” response, which can make them react more intensely to minor irritants2.
Understanding and managing these reactions can involve recognizing personal triggers, learning stress-reduction techniques, and finding healthier ways to express emotions. If you notice a pattern of getting angry over little things, it might be helpful to explore these feelings further, possibly with the help of a professional, to find more constructive ways to deal with them3.
People may develop a short fuse because they have experienced long stretches of time of being ignored or treated unfairly, and they were only able to feel safe or stand up for themselves by using anger and aggression. The reasons why some people may have a shorter temper than others can be quite varied and complex. Here are some factors that can contribute to a shorter fuse:
Genetic Influence: Genetics can play a significant role in a person’s personality traits, including their predisposition to being short-tempered1.
Neurophysiological Factors: The way our brains are wired can affect how we process emotions and react to stress, which can lead to a shorter temper1.
Childhood Development: Experiences during childhood can shape how one deals with anger and frustration later in life1.
Underlying Mental Health Conditions: Certain mental health disorders, such as intermittent explosive disorder (IED), anxiety disorders, depression, oppositional defiant disorder (ODD), bipolar disorder, and post-traumatic stress disorder (PTSD), can manifest as a short temper2.
Underlying Physical Health Issues: Physical health problems can also contribute to irritability and a short temper1.
It’s important to note that having a short temper can negatively affect both the individual and those around them. It can lead to strained relationships and can also impact one’s own physical and mental well-being. Recognizing the signs of a short temper and understanding its causes is the first step towards managing it effectively. Strategies such as stress management, assertive communication, and seeking professional help can be beneficial in coping with a short temper3.
Research shows that people who are more patient have higher well-being – more life satisfaction, hope, self-esteem, positive emotions in general. They seem to be able to pursue their goals with greater effort and have more satisfaction with their goal progress. Patience varies greatly among individuals, and several factors contribute to why some people appear more patient than others.
Here are a few reasons:
1. Emotional Regulation: Patient individuals often have better emotional regulation skills, allowing them to manage their feelings effectively and remain calm in frustrating situations1.
2. Life Experiences: People’s past experiences can shape their patience levels. Those who have faced and overcome many challenges may develop greater patience through their resilience2.
3. Personality Traits: Patience can be a part of one’s personality. Some people might naturally have a more patient temperament, which can be influenced by genetic factors and early life experiences2.
4. Cultural Influences: Cultural background can play a role in shaping patience. In some cultures, patience is highly valued and taught from a young age2.
5. Mindfulness and Perspective: Practicing mindfulness and having a broader perspective on life can help individuals become more patient. Understanding that some things take time and cannot be rushed is a key aspect of patience3.
6. Stress Levels: Lower stress levels can contribute to higher patience, as stress often reduces a person’s ability to wait calmly for outcomes1.
7. Goals and Motivation: People who are highly motivated and focused on their goals may exhibit more patience, as they understand that achieving significant objectives often requires waiting and persistent effort2.
It’s important to note that patience is a skill that can be developed over time. With practice and conscious effort, individuals can improve their patience, which can lead to better decision-making, relationships, and overall well-being4.
Impatience is not inherently negative; it can have both positive and negative aspects depending on the context and how it’s managed. While impatience is often associated with irritability and making hasty decisions, it can also be a driving force behind productivity and ambition1. Here are some perspectives on impatience:
Positive Aspects:
Motivation: Impatience can motivate people to take action and move forward with their goals2.
Productivity: A certain level of impatience can lead to increased productivity as it pushes individuals to complete tasks more efficiently1.
Change Catalyst: Impatience can be the catalyst for change, prompting individuals or groups to seek improvements and solutions2.
Negative Aspects:
Stress: Chronic impatience can lead to increased stress and anxiety3.
Relationship Strain: It can strain relationships if one’s impatience leads to conflict or misunderstandings4.
Rash Decisions: Acting on impatience can result in rash decisions with poor outcomes3.
Balancing impatience with the ability to wait when necessary is key. Understanding when to let impatience guide you and when to exercise patience can lead to better decision-making and overall satisfaction5. It’s about harnessing the energy that comes with impatience and directing it towards productive ends while being mindful of the potential pitfalls.
Being open to change makes it easier to adapt and view new challenges with less worry. Take care of yourself. Tend to your own needs and feelings. Do activities and hobbies you enjoy. Include physical activity in your daily routine. Get plenty of sleep and make bedtime rituals. Eat a healthy diet. Practice how to manage stress. Staying patient in challenging situations can be difficult, but there are several strategies that can help you maintain composure and patience:
1. Active Listening: Truly listen to what others are saying, which can help you understand their perspective and reduce frustration1.
2. Empathy Building: Try to see the situation from the other person’s point of view and acknowledge their feelings, which can foster patience and understanding2.
3. Establishing Trust: Building trust with others can lead to more open communication and a greater willingness to wait for outcomes2.
4. Problem-Solving: Engage in active problem-solving rather than focusing on the stressor, which can help you feel more in control and patient3.
5. Healthy Boundaries: Set and maintain healthy boundaries to avoid feeling overwhelmed, which can help preserve your patience3.
6. Time Management: Work on managing your time better to reduce the pressure of deadlines and the impatience that comes with them3.
7. Self-Care: Invest in self-care practices to reduce stress and improve your overall capacity for patience4.
8. Social Support: Reach out to friends, family, or professionals for support, which can provide relief and perspective4.
9. Positive Reappraisal: Reframe challenges as opportunities for growth, which can help you stay patient and motivated4.
10. Mindfulness: Practice mindfulness techniques to stay present and reduce the impulse to react impatiently5.
Remember, patience is a skill that can be developed over time, and utilizing these strategies can help you become more adept at handling challenging situations with grace and composure.
Impatience itself is not a direct cause of heart attacks, but it can be associated with behaviors and physiological responses that may increase the risk. For instance, impatience can be a component of a Type D personality, which is characterized by negative emotions like anxiety, irritation, and anger1. These emotions can lead to stress, which in turn may affect heart health.
Stress hormones, which can be elevated in individuals who are often impatient, have been found to stimulate platelets, making them more likely to clot in arteries that are already narrowed by heart disease. This process can potentially result in a heart attack2. Additionally, these hormones can cause the body’s fat cells to release fat into the bloodstream, which is another risk factor for heart disease2.
Moreover, a study has indicated that hostility, which can be a sign of impatience, was an independent predictor of dying from a second heart attack, after adjusting for other factors3. This suggests that managing negative traits such as anger and insecurity, which may be related to impatience, could be beneficial for heart health1.
It’s important to note that while impatience and associated stress can contribute to cardiovascular risk factors, they are just one part of a complex interplay of genetic, behavioral, and environmental factors that affect heart health. If you’re concerned about your heart health, it’s best to consult with a healthcare professional for personalized advice.
Stress can lead to negative emotions when it overwhelms an individual’s ability to cope. Here are some types of stress that commonly cause negative emotions:
Routine Stress: This comes from the pressures of daily responsibilities like work, school, family, and other routine activities.
Sudden Negative Change: Events like losing a job, divorce, or financial troubles can lead to acute stress.
Traumatic Stress: Experiencing or witnessing a dangerous, shocking, or life-threatening event can cause this type of stress.
Chronic Stress: This occurs when a person faces continuous challenges without relief or relaxation between stressors, leading to a negative emotional state.
Self-Induced Stress: Sometimes, negative self-talk, unrealistic expectations, or perfectionism can induce stress.
Environmental Stress: Living in a chaotic or unhealthy environment can contribute to chronic stress.
Each type of stress affects individuals differently, and what may be stressful for one person might not be for another. It’s important to identify the sources of stress and develop coping strategies to manage its impact on emotional well-being.
The relationship between negative emotions and disease is a complex one.
Research has shown that while negative emotions can be adaptive and beneficial in certain contexts, such as responding to immediate threats or challenges, chronic negative emotions may have a detrimental impact on physical health.
For instance, a study suggests that contextually sensitive negative emotions can be adaptive and associated with better psychological health and adjustment1.
However, chronic stress and negative emotions have been linked to suppression of the immune system and may contribute to the onset of various illnesses, including cardiovascular and gastrointestinal issues, fatigue, hypertension, diabetes, and even certain autoimmune diseases23.
It’s important to note that while negative emotions can contribute to disease, they are not the sole cause.
Many factors, including genetics, lifestyle, and environmental influences, play a role in the development of diseases.
Therefore, it’s essential to consider the broader context when examining the impact of emotions on health. Search Images (bing.com)
Positive coping strategies are techniques that help individuals manage stress and navigate through challenging situations in a healthy and constructive manner. Here are some effective positive coping strategies:
Establishing and maintaining boundaries: Knowing your limits and communicating them to others can prevent stress from overwhelming situations1.
Practicing relaxation strategies: Techniques such as deep breathing, meditation, and mindfulness can help calm the mind and reduce stress2.
Getting regular physical activity: Exercise is a great way to relieve stress and improve mood2.
Making to-do lists and setting goals: Organizing tasks and setting achievable goals can provide a sense of control and purpose2.
Engaging in problem-solving: Taking steps to address the source of your stress can provide relief and a sense of accomplishment2.
Seeking social support: Talking to friends, family, or professionals can provide comfort and practical solutions1.
Positive thinking and journaling: Reflecting on positive aspects and writing down your thoughts can help shift focus from stressors3.
These strategies can be tailored to individual needs and preferences, and incorporating them into daily life can significantly enhance one’s ability to cope with stress. It’s also beneficial to explore different strategies to find what works best for you.
Practicing mindfulness involves a set of techniques that help you focus on the present moment, often leading to a sense of calm and clarity. Here are some practical steps to get started:
Choose a quiet and comfortable place to sit or lie down.
Set a time limit if you’re just beginning, such as 5 or 10 minutes.
Pay attention to your breath. Notice the sensation of air flowing into and out of your body.
Notice when your mind wanders from your breath. This is normal, and when you notice this, gently return your focus to your breathing.
Adopt a non-judgmental attitude. Try not to judge yourself for any thoughts or feelings that arise. Simply observe them and let them pass.
Expand your awareness gradually. After focusing on your breath, move your attention to other sensations in your body, then to sounds, and eventually to your thoughts and emotions.
You can also incorporate mindfulness into daily activities like eating, walking, or even during work. The key is to be fully engaged in the here and now, paying attention to the details of your actions and sensations without judgment.
For more structured practice, you might consider guided meditations for mindfulness exercises available in books, apps, or online resources123.
Meditation can be a wonderful way to relax and find balance.
Here are some meditation techniques that are suitable for beginners and can be easily incorporated into your daily routine: Search Images
Breathing Meditations: Focus on your breath, the inhalation and exhalation, to anchor your mind in the present moment1.
Mindfulness Meditations: Be fully present, observe your thoughts and sensations without judgment, and gently bring your attention back to the present whenever it wanders1.
Focus Meditations: Choose an object of focus, such as a candle flame or a mantra, and return your attention to it each time you notice your mind drifting1.
Movement or Walking Meditations: Integrate mindfulness into movement, paying close attention to the sensations of walking and the rhythm of your steps1.
Mantra Meditations: Repeat a calming word or phrase to help focus the mind and foster a sense of peace1.
Loving Kindness Meditation: Cultivate feelings of compassion and love by directing well-wishes towards yourself and others1.
Body Scan Meditation: Progressively relax different parts of the body, starting from the toes and moving upwards, to release tension and stress2.
These techniques can help you start a meditation practice and discover what works best for you. Remember, the key to meditation is consistency, so try to make it a regular part of your daily routine. Happy meditating!

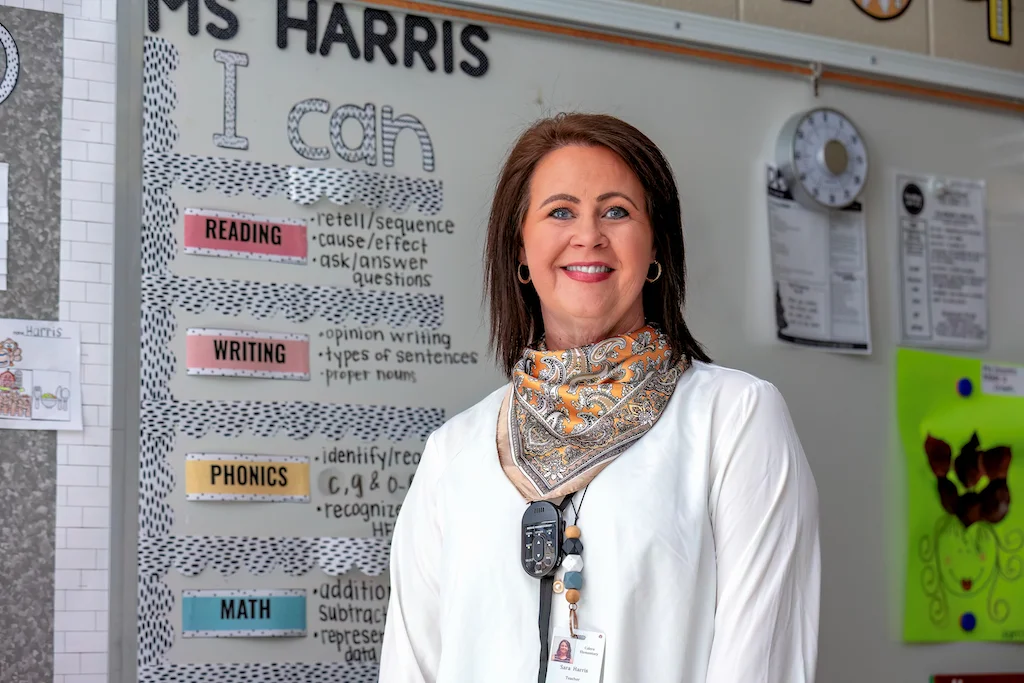









.jpg)


 Down from the “for-lifer” friends disappearing on you to you feeling disconnected from your healthy peers and loneliness.
Down from the “for-lifer” friends disappearing on you to you feeling disconnected from your healthy peers and loneliness.  I hope and pray she reaches full recovery in Jesus name.
I hope and pray she reaches full recovery in Jesus name.