

By Elliott Freed
4 Questions that May Change Your Mind about Vaccines.
Legal Disclaimer: This article is not intended to diagnose, treat or cure a disease. Nor is it intended as medical advice.
The reader is responsible for their decisions and their health.
Vaccines are a difficult issue for many people to discuss. Some people become highly charged and either defensive or aggressive when discussing them.
The public dialogue seems polarized.
On one side are the small but vocal group of people who raise concerns about vaccines. Most of these people are parents with vaccine injured children, the scientists who study vaccine injury and the doctors who treat these children.
On the other side is the news media who shut out their stories and the seeming majority of the public. I have heard more than a few stories of family members cutting off relationships when they found out there was a vaccine injury.
Rather than listen to their child or sibling and be forced to question their
faith in vaccines and the establishment that creates and administers them,
they simply cut the family in half.
It is my belief that most people are open to the truth in a less emotionally charged way. They are curious what the hubbub is about but do not feel comfortable speaking publicly because of the intensity of the response
from the more vocal elements in the conversation.
We don’t have any great love for the government and industry. It would not surprise us to discover they are up to shenanigans yet again. It seems par for the course. But we more or less trust our doctor. For us to bother questioning them and doing our own research on a routine medical procedure usually requires some kind of major trauma or shock.
In doing the research summarized in this article I have met many families who have experienced that trauma and shock through vaccine injury. In some cases the child died.
A couple years ago a dear friend lost her two month old child to vaccination.
This was confirmed by three separate pathologists and a six month police investigation.
How is it that there is a clear, scientific, legally recognized way to determine when a child dies from a vaccine yet the vast majority of the public and even most doctors insist it is not possible?
If the scientifically and legally established fact that vaccines can kill a baby is not known by the public or acknowledged by doctors, what else about vaccines remains hidden in plain view?
This article is for those who want the facts, regardless of their personal or social ramifications.
We introduce the important questions about vaccines. What does the clearly documented historical record say about their role in the decline of infectious diseases? What is known about the dangers of vaccines? When considering
the cost-benefit ratio of vaccines, what questions must we ask?
This issue is very complicated and not easy to understand. Please approach
it with an open and curious mind, yet also with a healthy dose of skepticism.
There is a lot of heavy fire power at play in this conversation. As you contemplate these questions and search for answers, stay low to the ground. Think like a scientist. Ignore the declarations and look at the data. Look at what is happening and look for the science that explains what is happening.
Be skeptical of the people who deny what is happening. And look out for confirmation bias and financial interests.
Editors in chief of three of the four leading medical journals in the world have spoken and written publicly about the unreliability of medical science and the way it is more of a social phenomenon than a scientific one. Medical science has long been skewed by the profit motive. [1]
Without further ado, here are the questions to begin considering.
Question #1: Did vaccines save us from the deadly pandemics?
The United Kingdom was the first country to keep data on mortality from infectious diseases in 1838. The U.S. began in 1900. Other countries have
other time frames but the trends are roughly similar.
In the U.K. some of the biggest killers of the 19th century were scarlet fever, typhoid, cholera, measles and whooping cough, also known as pertussis.
Small pox was statistically more rare.
The only vaccine available in the 19th century was for smallpox.
Invented by Edward Jenner in 1796, throughout the 19th century it was
always associated with outbreaks of small pox. Most of the people who died of smallpox in these outbreaks had been vaccinated. In 1885 the city of Leicester turned away from vaccination and embraced quarantine and sanitation.
Smallpox virtually disappeared in Leicester within a couple years.
Within a decade quarantine had replaced vaccination throughout
the country and by 1902 small pox was very rare in the U.K.
Quarantine is now the preferred method of containing infectious outbreaks.
Its how we dealt with SARS and Ebola. It is also how we eradicated small pox around the world. While people credit vaccines, they were only one part of the eradication drive. When cases were identified they were quarantined and vaccinated. Much of the world never had extensive small pox vaccination campaigns.
Cholera, typhoid and scarlet fever are all now very rare in the first world.
There are no vaccines or significant vaccine campaigns for any of them.
They faded for other reasons.
In the U.K. the death rate for whooping cough had declined by 99.74% by the time the vaccine became common in the 1950s. The death rate from measles had declined by 99.96% by the time the vaccine was introduced in 1968.
In the U.S. we see from C.D.C. data, culled from a study published by the AMA, that the death rate from infectious diseases had bottomed out by the time vaccines were being used. It has not changed significantly in the past 65 years, since before the polio vaccine was introduced. [2]
Even the tale of polio is more complicated than first meets the eye. Polio was the diagnosis given to anybody presenting with acute flaccid paralysis (AFP) for 24 hours. There were about a thousand cases a year in the U.S. up until 1943. From 1943 to 1952 cases of AFP skyrocketed. They all received the diagnosis of polio. Most people recovered beginning within one to two weeks of onset. A few did not. In the worst year, 1952, about 3,500 people in the U.S. succumbed to AFP, called polio at the time.
During this time there was a lively debate among the scientific community about what was causing the outbreak of AFP. While there was strong evidence that it was DDT the money and publicity behind the viral theory won out.
Despite the public victory, by 1952 it was becoming clear that DDT was the likely culprit. Invented in the late 19th century as a nerve gas chemical weapon, in 1938 it was repackaged for use as a mosquito killer. It was applied liberally from 1943 through 1952 on swimming pools and school cafeterias full of children.
While there has never been a public admission that DDT was responsible for the outbreak of AFP, in 1953 they stopped spraying it on children. In two years the rate of AFP dropped by one third. The next year the death rate dropped by half. Today DDT is illegal in many countries, including the U.S.
In April, 1955, the polio vaccine was introduced. Cases of paralysis increased, largely among the vaccinated. But diagnostic criteria were changed for “polio.” Instead of 24 hours one had to be paralyzed for 50 to 70 days and the C.D.C. themselves had to find the polio virus in the stool.
Cases of “polio” virtually disappeared while cases of AFP went uncounted.
Today the C.D.C. does not keep track of cases of AFP. [3]
Thus “polio” was eradicated but we still have roughly the same level of AFP
as we had before 1943. There are now dozens of known causes of AFP and a
few people with the symptom have the polio virus. Many people point to the eradication of polio in India that has been talked of in the media as proof the vaccine is working.
Again, we have to look more closely.
According to the WHO, the rate of AFP has increased about 1,000 percent
in India since the vaccination campaign began. They call it “non polio” AFP because everybody has been vaccinated. This assumes the vaccine works.
As we saw in the U.S. it actually is causing more paralysis. Dr. Jacob Puliyel
is the head of pediatrics at St. Stephens Hospital in Delhi, India and a member of the National Technical Advisory Group on Immunization of the Government of India. In February of 2015 he published a study in the leading pediatric medical journal in the world. He found that the 10 fold increase in paralysis was due to the polio vaccine. Not only that, the case fatality rate was higher as well, so it was a more deadly form of AFP than whatever people had before.
Did we eradicate “polio?” Maybe. But at what cost?
We increased paralysis 10 fold and the death rate even higher.
This should give one pause.
When people, even the government or the spokespeople for the vaccine manufacturers themselves make declarations that vaccines have saved millions of lives, ask for the hard data. Clearly in the U.K. & in the U.S. and with “polio” in India, this is not the case, even according to the data from the people making the claims. [4]
Question #2: If vaccines are not saving us from deadly pandemics,
are they at least protecting us from getting the illnesses and thereby improving our health?
While the data on deaths from infectious diseases is pretty cut and dry,
at least in the cases mentioned above, this question is more complex.
Vaccines cause diseases. That is the whole point of vaccines.
The theory is they cause a mild form of the disease that prepares the body to fight off the more severe natural form later. When somebody uses the phrase, “vaccine preventable disease,” proceed with caution. There is no such thing. Vaccines are intended to cause diseases. It is quite likely that anybody who does not know this may also not know other important things about vaccines. When we vaccinate we are choosing the vaccine version of the disease over the natural version.
In considering the cost-benefit analysis of vaccine induced diseases we have to consider a few key points. I summarize them here:
1) Inherited immunity.
When a woman gets a disease like measles or mumps naturally, she develops a wide variety of immune factors that she passes to her child in the womb and through breast milk. So far over 100,000 have been identified and there are likely far more yet to find. These accumulate generation after generation.
When she gets the vaccine version of the disease she does not develop the wide range of immune factors and cannot pass them to her children.
This means the children are more susceptible to infection and it means that centuries of cultivated natural immunity are lost in vaccinated families.
2) Long term benefits of viral diseases.
There is growing evidence that childhood viral illnesses are important for the development of adult health. There are scientific studies showing how they reduce rates of some cancers and heart conditions.
There are also new cancer treatments using viruses. This raises the question:
If they can treat it could they have a role in preventing it?
And there are endless anecdotes from mothers who noted significant developmental leaps in their children following viral diseases.
There is far more we don’t know about how viruses work in the body than we do know. What other long-term benefits are we losing?
3) Vaccine ingredients.
The public dialogue has focused on mercury in vaccines. Much of it has been removed but the total dose may have risen as it is in many flu shots which are recommended yearly. It is also in some pertussis vaccines as well as a few others. There are other ingredients which must also be considered. Human fetal tissue, monkey kidneys, aluminum, formaldehyde, detergents that break down the blood brain barrier and other industrial chemicals and animal byproducts are in vaccines.
The well established toxicology of each of these is too extensive to cover
in this short article. People sometimes argue that the doses are small.
The doses of many pharmaceutical drugs are equally small but are still recognized to have significant effects on our biochemistry.
Furthermore, if we can observe the known effects of these chemicals and animal and human tissues in people who have been injected with them, we have to consider their causative role.
Others argue that we eat more of these chemicals than we inject.
This is true but we have a digestive system to protect us from the toxic material we eat. All food would be toxic if injected, yet we ingest it with impunity many times a day. When we inject something it does not go through the normal pathways to be broken down.
For example, 99.5% or more of the aluminum we eat passes through us in our stool. The tiny amount that does get absorbed is rapidly excreted through the kidneys. 75-100% can remain in us indefinitely when injected. It is for this reason that it is used in vaccines. It binds to the pathogens and keeps them in the body indefinitely. This keeps the antibody levels up. Aluminum is known to disrupt nearly all healthy biological functions.
Another example is formaldehyde. Formaldehyde is rapidly broken down when we eat it. Like the human fetal tissue, monkey kidneys and other animal parts in vaccines, it can remain in its whole form when injected.
The types of cancer now common among children are the types most closely associated with formaldehyde.
This leads to the question, with all these toxins, are vaccines safe?
Before injecting these chemicals into your children, read up on their toxicology and consider the cost-benefit ratio between the natural form of the disease and the manufactured version.
Question #3: Are vaccines safe?
When vaccine manufacturers were on the cusp of bankruptcy due to an unsustainable number of lawsuits and the damages they had to pay out,
in 1986 congress passed a law absolving them of all legal liability from
the known negative effects of their products.
This law was further strengthened in 2011 when the Supreme Court found that vaccines are unavoidably unsafe and manufacturers are under no obligation to make them safer.
As part of the 1986 law the Department of Health and Human Services maintains the Vaccine.
Adverse Events Reporting System (VAERS).
This is a passive reporting program that is thought to capture a very low percentage of total adverse events. Nonetheless there are tens of thousands of reports filed every year. What are the real numbers? With a passive reporting system we’ll never know. Why are we not making a greater effort to count these cases and how can a doctor feel comfortable saying vaccines are safe if they are full of toxins and we are not studying the reactions people are having to them?

US COVID-19 Vaccine Progress Tracker | Vaccinations by State | USA Facts
HHS also runs the National Vaccine Injury Compensation Program:
which has paid out to the families of vaccine injured children nearly four billion dollars in damages as of this writing.
As part of this court program they maintain the Vaccine Injury Tables. This is a list of injuries that are uncontested and recognized as clearly due to vaccines. In theory these injuries are immediately compensable. The list includes brain damage, paralysis, arthritis, death and more. Other injuries have to be more convincingly demonstrated in court.
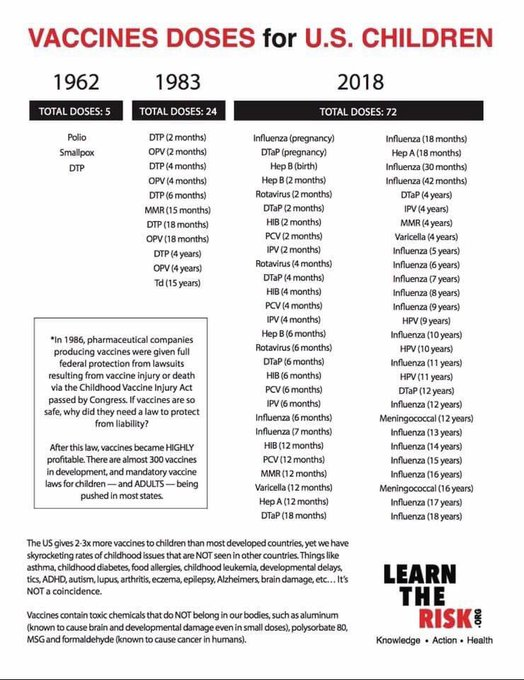
This freedom from liability ushered in the era of growing vaccination recommendations and requirements. These new recommendations include yearly flu shots and the chicken pox and hepatitis B shots. The flu vaccine was invented in the 1940s. The chicken pox vaccine was invented in the 70s. The hepatitis B vaccine was invented for use by prostitutes and drug addicts who might be sharing needles. After legal liability was removed, hep B was recommended for all newborn babies on the day of their birth, flu shots were recommended yearly and the chicken pox shot was recommended as well.
There is now a plan being implemented by the Department of Health and Human Services to get all children and adults up to speed on all vaccines.
While I got three shots as a kid in the 70s, there are now dozens of shots required for children to enter kindergarten. Since the early 90s when we began ramping up this liability free experiment on the immune systems of our children with dozens of doses of known, well documented neurotoxins combined with cancer causing chemicals we have seen steadily rising rates of immune system diseases and neurological diseases as well as a growing pandemic of cancer among children.
While the government and media have focused the research and public dialogue on a handful of their own questionable epidemiological studies that failed to find a statistical link between one vaccine, the MMR (measles, mumps and rubella), and one behavioral diagnosis, autism, the research is rolling in from around the world on the whole range of biological malfunctions and ailments caused by vaccines and their ingredients.
These include brain damage, epilepsy (one in 20 American kids), multiple sclerosis, genetic disruption, immune system diseases, asthma, allergies, diabetes, learning disabilities and developmental delays, food allergies and many more.
The C.D.C.’s response is to ignore all this data and focus on denying the link between the MMR vaccine and autism. The industry responds by developing new vaccines for the diseases caused by the old ones. There are now hundreds of “vaccines” in development that have nothing to do with infectious diseases. They are liability free and state governments mandate them. The media discusses the studies that “fail to find a link” between MMR and autism and ignores all the ones that do find a link between vaccines and all manner of ailments. When they pronounce that vaccines have been proven to be safe they are ignoring all this evidence and declaring the science settled without having read it. And the public cries out for them because they are afraid of polio, in all likelihood a misdiagnosis of industrial neurotoxicity. A better business model would be hard to come by.
Question #4: What is the true cost benefit ratio of vaccines?
Once we realize that vaccines are not responsible for reducing deaths
from infectious diseases we must evaluate them more closely. [5]
Have they reduced incidence of infectious diseases?
It appears that way until we think more deeply. Official statistics may show declines in rates of infectious diseases but when we understand that everybody who receives the vaccine gets the manufactured version of the disease, we have to look more closely. We have replaced the natural infectious diseases which were already slowly fading away with the manufactured variety that every child now has injected into them multiple times before they begin kindergarten.
Through this process thousands of years of inherited, cultivated immunity
are lost. The long term developmental and health benefits of natural viral infections are lost. The brain may be damaged. The immune system may be further handicapped. We must therefore be more astute in our cost-benefit analysis.
Conclusion:
This article is not intended to sway a reader one way or another to accept or reject vaccines. It is intended to encourage the reader to study more deeply.
Vaccination is a complex issue. The historical data and published science are sufficient to keep one busy, let alone the social conversation and the broader implications of what one might learn. It can take the curious student a year or two of study to develop a basic understanding of the issue. Is there a way to speed up the process?
We recommend a series of three books that make up an introductory course.
Vaccination 101 if you will. All three of these books are well sourced.
The first book is Vaccine Primer: An Inoculation, by yours truly. It is a concise book that lays out the parameters of the discussion, asks the important questions and introduces us to the relevant information.
This book can be read in a couple hours.
The second book is, Dissolving Illusions by Dr. Suzanne Humphries and Roman Bystrianyk. Dr. Humphries is a nephrologist and medical school professor who has dedicated the last few years to vaccine research.
Mr. Bystrianyk has been involved in recovering children from vaccine injury for decades. This book goes into greater historical and scientific detail. It cites over 800 sources, many of them peer reviewed science or seminal works of medical history.
Finally, read the book, Vaccine Safety Manual by Neil Miller. This book goes through each vaccine. Citing over 1,000 scientific studies it covers the disease, its natural history, the development of the vaccine and the associated follow up science.
Please: When somebody close to you shares their story of vaccine injury, listen. It is real. It is far more common than we are led to believe. And the U.S. govt. well documented history, and the science itself do in fact back up their story.
References:
[1] Dr. Marcia Angell was the Editor in Chief of the “New England Journal
of Medicine” for many years. She has written a book on the problems with medical science. She is now a professor at Harvard.
She wrote this article on the subject of corruption within medical science.
Dr. Richard Horton is the editor in chief of the world’s leading medical journal, The Lancet. Writing in his own journal he states that
medical science has “taken a turn towards darkness.”
The former editor in chief of the BMJ (formerly the British Medical Journal) writes about his attempts while editor to evaluate the process
of peer review.
This web page has links to more articles about the issue of ethics
in medical science, medical education and the practice of medicine.
[2] This page from the C.D.C. The website discusses the decline in infectious diseases in the 20th century. They give due credit to sanitation. They also credit vaccines, but if you look at Figure 1, the chart halfway down the page, the data tell a more clear picture of the role of vaccines. The DTP was introduced in the late 40s. The MMR was introduced in the 60s. Note the difference between the data and the declarations.
[3] This is an article posted to the website of the C.D.C. in October, 2014.
It discusses cases of AFP in California. In the second section of this report, “Discussion,” it is noted that the C.D.C. does not record cases of AFP.
[4] This web page offers more links to scientific and historical literature on polio, along with some analysis.
[5] We’ve already discussed the role of vaccines in the U.K., the U.S. and the case of “polio” in India.
This chapter of this book explores the origin of the claim that the measles vaccine has saved millions of lives. On pages eight and nine are data on death rates of children under five in Africa and India from 1950.
They show how the introduction of vaccines affected those rates.
Here is data on deaths from infectious diseases in the U.K. between 1838 and 1978. Note: the major declines that occurred before vaccines were introduced.
Also note that there is no vaccine for scarlet fever.
Autism and Childhood Vaccinations: Do Vaccinations Put Children at Increased Risk to Develop Autism?
~
Childhood Vaccines and Autism | C-SPAN.org
Witnesses testified about potential links between vaccines and childhood autism. Among the topics they addressed were current research into the problem, the potential scope of the disease, and evaluations into
the severity of the problem.
Vaccines VS Variant: State of Texas Study (Pfizer, Moderna, Johnson & Johnson)